Introduction
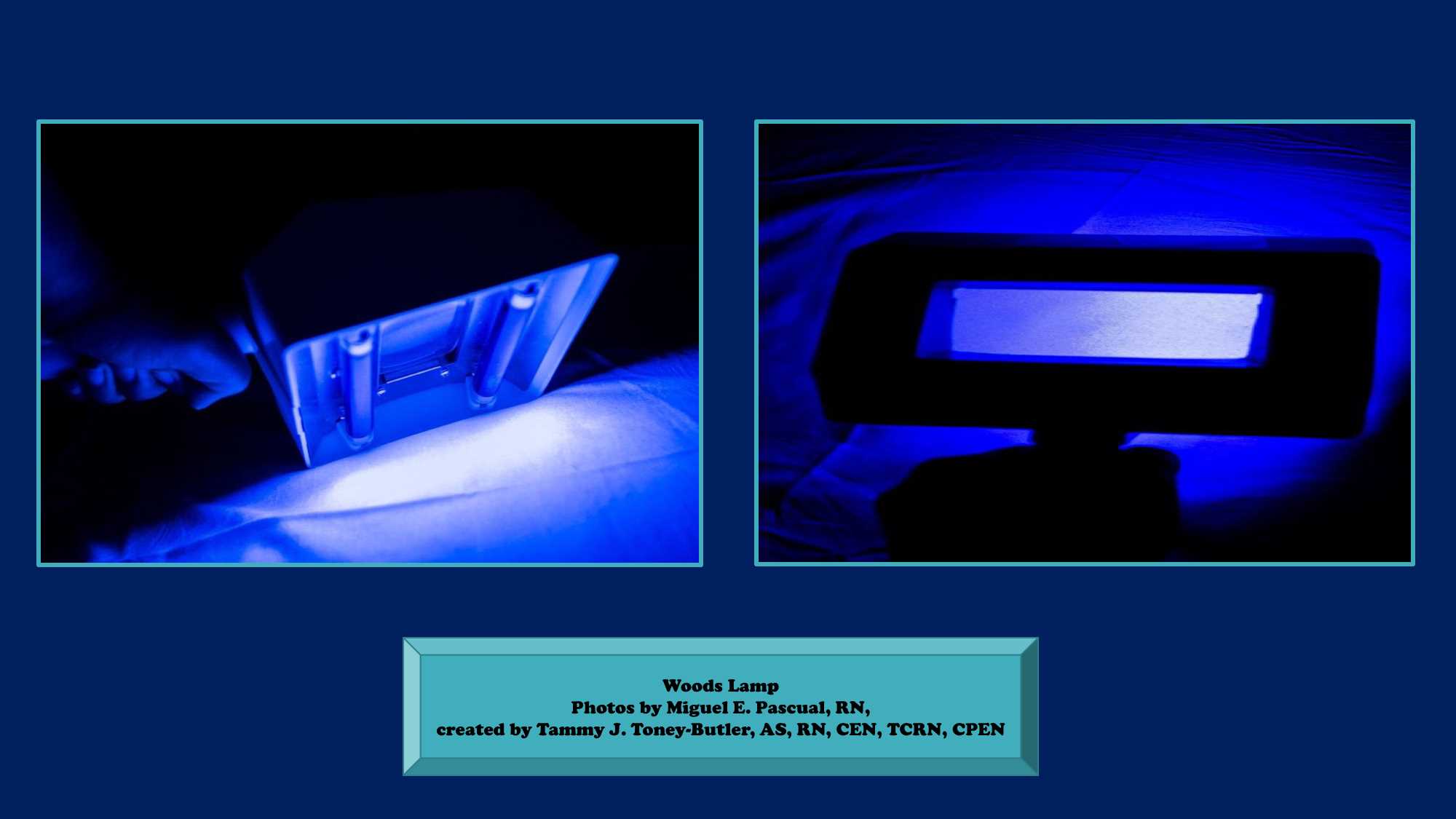
American physicist Robert Wood developed what is now known as the Wood's light or Wood's lamp. Wood's lamp is a source of long wave ultraviolet light and can be used to detect the fluorescence in skin and hair, which is a feature of some dermatophytes. It has diagnostic utility in the detection of inconspicuous scalp lesions. Apart from its use in the diagnosis, the Wood's lamp can be used to select infected skin and hairs for laboratory investigation. It also can detect disorders of skin pigment, including vitiligo and other skin irregularities. The lamp can also be used to determine if the patient has a corneal abrasion on the surface of the eye.[1]
Normally, the light will appear purple or violet, and the skin will not fluoresce. However, certain bacteria, fungi, or changes in pigmentation of patient skin will cause the affected area of the skin to change color under light; hence this is used for inspection and detection of certain fungal infections. Wood's light is not a therapeutic or treatment device.[2]
The room needs to be completely dark before the use of Wood's light to create the dermal illumination. This test is performable by any healthcare worker, but to properly interpret the findings, it is best if a dermatologist or other experienced provider administers the test.[3]
Indications
The Wood's lamp can detect areas of skin that are pigmented or depigmented and can also detect fluorescence. Normal healthy skin appears as a blue color but may show white spots when the skin is thick and yellow when it is oily. Purple spots indicate dryness or dehydration. Clothing lint is often bright white and shiny.[4]
A positive result is when there is a pigmentary disorder that is obvious, or the fluorescence is noted. The Wood's lamp is often used to make a diagnosis of the following skin disorders:
- Disorders of pigmentation like melasma, vitiligo
- Pityriasis Versicolor presents as a rash on the chest or back - the rash will emit an orange glow.
- Tinea capitis will reveal areas of baldness, and the Microsporum species will fluoresce blue-green - however, many other fungal infections may not fluoresce with Wood's lamp
- Scabies and head lice
- Erythrasma is caused by Corynebacterium, which presents as a coral red pigmented rash in the skin folds
- Pseudomonas, which will fluoresce green
A Wood's lamp is also used to look for signs of porphyria in erythrocytes, stool, and urine. Sometimes beauticians may assess for skin imperfections and signs of aging with a Wood's lamp. When a slit lamp is unavailable, the ophthalmologist may use the Wood lamp to search for scratches and foreign bodies in the cornea.
Physicians often use the wood lamp to examine for fungal, bacterial, and parasitic infections.
The Wood lamp is safe and does not damage the skin or cause sunburn. The examination is usually very brief and unlikely to cause harm even to light-sensitive individuals. The recommendation is for patients to close their eyes when during exposure to a Wood's lamp.[5]
Contraindications
No obvious contraindication exists to the use of Wood's light to check the patients for any skin infection or pigmented disorders. Patients need to have their eyes covered to avoid any risk to the cornea.[6]
Equipment
To use Wood's lamp, the skin to be examined should not be recently washed; it must be free of makeup, deodorant, moisturizing cream, or any other topical lotion. These topical liquids can cause a false positive test. Turn on the Wood's lamp for about 60 seconds, and the room must be dark. Then examine the skin with Wood's lamp for a few seconds. The lamp is usually held 10-30 cm away from the skin and does not emit heat. The exam is painless.[6]
Personnel
Dermatologists are the most common users of the device, but all health care providers should know how to use it in the clinic especially general practitioners. The procedure is not challenging to administer but the interpretation of the result requires training and experience.
Preparation
There is no specific protocol needed for the patients undergoing Wood's light. It is essential to advise the patients not to wash their faces before examining them with Wood's light.
Technique or Treatment
The Wood's light or lamp is often used to make a diagnosis of specific skin and hair disorders. By exposing human tissues to the light emitted by Wood's lamp, one can determine the cause. Wood's lamp emits black light which is invisible to the naked eye because it is in the ultraviolet spectrum. The lamp glows in dark environments because it also emits some light in the violet region of the electromagnetic spectrum. The traditional Wood's lamp is covered with a wood filter and emits wavelengths in the 320 to 450 nm range.[7]
Today, there are several types of Wood's lamps on the market that filter out visible light. The medical Wood's lamp contains a magnifying lens, a variety of phosphors with different peak emissions, white light, and black drapes to exclude ambient light.[8]
Complications
Complications associated with the use of Wood's light include:
- Wrong interpretations
- False positive or negative result
- Eye problems in cases of using the device for a long time without utilizing protective goggles
Clinical Significance
A Wood's lamp examination is a diagnostic test used in the diagnosis of many dermatologic disorders including:
1. Pigmentary disorders: Hypopigmentation or depigmentation, hyperpigmentation, and melasma.
2. Cutaneous infections:
- Fungal causes; Tinea versicolor, Pityrosporum folliculitis, and Tinea capitis.
- Bacterial causes; Corynebacterium minutissimum, Pseudomonas species, and Propionibacterium acnes.
3. Porphyrias
There is a modern version of Wood's light which has a wavelength of 395 nanometers and is mainly concerned with skin and appendageal tumors like basal cell carcinoma and actinic keratosis. Also, it can be used to detect certain benign conditions like milia and comedones.
Enhancing Healthcare Team Outcomes
Wood's light is a simple and effective method to diagnose specific dermatosis including cutaneous fungal, bacterial infections, and pigmentary disorders. The test is done in the clinic under the direct supervision of the treating provider. In certain situations, it is not enough to do Wood's light test since the result is equivocal or the case is complex. Because the Wood's light emits light in the ultraviolet range, it is prohibited to look at the light for a long time; both patients and the physician need to protect their eyes.