The triceps brachii is a large, thick muscle on the dorsal part of the upper arm. It often appears in the shape of a horseshoe on the posterior aspect of the arm. The primary function of the triceps is the extension of the elbow joint. It is composed of three heads (tri = three, cep = head): a long head, a lateral head, and a medial head. The tendons all have different origins, but the three heads combine to form a single tendon distally.
The long head originates from the infraglenoid tubercle of the scapula, while both the lateral head and the medial head both originate from the humerus. The three heads converge into a single tendon, which attaches to the proximal portion of the olecranon process (the bony prominence of the elbow) located on the upper portion of the ulna.[1]
Structure and Function
The triceps' primary function is extending the forearm at the elbow joint, which opposes the action of the flexors such as the biceps brachii. At rest, with the arm slightly bent with flexion, the biceps brachii overpowers the triceps brachii. Along with extending the forearm at the elbow joint, the triceps can also stabilize the elbow joint when the forearm and hand are doing fine movements such as writing.[2][1]
The triceps brachii is located in the dorsal compartment of the arm. The lateral intermuscular septum separates the dorsal part of the arm from the ventral aspect, which is where the flexors of the arm are (biceps, brachialis, and brachioradialis).
Long head—The origin of the long head is the infra-glenoid tubercle of the scapula. Because it attaches to the scapula, the long head not only extends the elbow but will also have a small action on the glenohumeral or shoulder joint. With the arm adducted, the triceps muscle acts to hold the head of the humerus in the glenoid cavity. This action helps prevent any displacement of the humerus. The long head also assists with the extension and adduction of the arm at the shoulder joint. The lateral head is also active during the forearm extension at the elbow joint when the forearm is supinated or pronated.
Medial head—The origin of the medial head is at the dorsal humerus, inferior to the radial groove and connecting to the intermuscular septum. The medial head does not attach to the scapula and therefore has no action on the glenohumeral joint, whether with stabilization or movement. However, the medial head is active during the forearm extension at the elbow joint when the forearm is supinated or pronated.
Lateral head—The lateral head originates at the dorsal humerus as well, but unlike the medial head, it is superior to the radial groove, where it fuses to the lateral intermuscular septum. This head is considered to be the strongest head of the three. It is active during the extension of the forearm at the elbow joint when the forearm is supinated or pronated.[3]
Embryology
The mesoderm develops during the third week following the gastrulation process. In the third week, the paraxial mesodermal layer begins to organize into segments called somitomeres. These consist of concentric layers of mesodermal cells formed with cranial to caudal progression. Subsequently, they organize in somites. The somites appear with a frequency of about three pairs a day so that at the fifth week are recognizable 42 to 44 pairs of somites, of which there are four occipital pairs, seven cervical, twelve thoracic, five lumbar, five sacral, and between eight and ten coccyx pairs.
The triceps brachii begins to develop during the fifth week of embryogenesis. The muscle originates from the dorsal muscle mass of the upper limb bud and is derived from the paraxial mesodermal leaflet.[4]
Blood Supply and Lymphatics
The arterial supply to the triceps is provided by the deep brachial artery, which is a branch of the brachial artery and is supplied by ulnar collateral arteries.[5] The venous drainage is the brachial vein that runs with the deep brachial artery.
Lymphatic vessels, like lymph nodes, are divided into superficial and deep. The superficial lymphatic collectors are the cutaneous lymphatic capillaries, especially of the hand, from which they course proximally in the forearm to form three groups: medial, lateral, and anterior collectors. In the arm, then they continue to get to the armpit to the axilla.[6]
Nerves
The provision of nerve supply to the triceps is by the radial nerve (root C6, C7, and C8). However, according to the cadaveric study, it was found that the medial head of the triceps brachii could be innervated partially by the ulnar nerve. Following that line of investigation, other research also reveals that the long head of the triceps brachii can also be innervated partially by the axillary nerve.[7]
The radial nerve originates from the posterior cord of the brachial plexus in the anterior axilla. The nerve then courses along with the profunda brachii artery (the artery that supplies blood to the posterior arm) and travels through the arm inferolaterally. It passes behind the humerus and through the radial groove between both the lateral and medial heads of the triceps brachii.[8]
Muscles
Triceps brachii
Long head
Origin: infraglenoid tubercle of the scapula
Insertion: olecranon of ulna
Action: extension of the forearm
Innervation: radial nerve
Lateral head
Origin: posterior aspect of the humerus, superior to the radial groove
Insertion: olecranon of ulna
Action: extension of the forearm
Innervation: radial nerve
Medial head
Origin: posterior aspect of humerus, inferior to the radial groove
Insertion: olecranon of ulna
Action: extension of the forearm
Innervation: radial nerve
Physiologic Variants
There have been reports of a fourth head in a few cadaver studies. This accessory muscle can originate from the humerus, shoulder capsule, coracoid processes, or muscles in close proximity. These accessory muscles can potentially compress the radial and ulnar nerves. Therefore, it is essential for surgeons and physicians to keep in mind that although rare, these variations exist, which can help diagnose cases of nerve entrapment and other pathologic causes that may not be explained by any other typical factors.[9][10][4]
Surgical Considerations
Axillary nerve damage can have an impact on the long head of the triceps brachii (LTB). Therefore, people with axillary nerve damage should undergo an assessment for the function of the LTB. If they demonstrate lost function, this shows a poor prognosis, and early repair at three months is recommended.[11]
The triceps muscle can undergo reinnervation through a distal nerve transfer. Commonly used nerves for reinnervation include the flexor carpi ulnaris fascicle of the ulnar nerve and the posterior branch of the axillary nerve. Both of these nerves have been shown to recover the function of the triceps muscle[12]
Additionally, various heads of the triceps can be used as flap coverage in traumatic injury. The medial and lateral heads are commonly harvested as flaps. These procedures are indicated during nerve injuries, shoulder or elbow defects, or muscular reanimation.[13]
Clinical Significance
The triceps reflex, elicited by sharply striking the triceps tendon, is often used to test the function of the nerves of the arm. This reflex tests spinal nerves C6 and C7, predominately C7. The reflex is tested by abducting the patient's shoulder and elbow to 90 degrees. Then the triceps tendon is tapped using a reflex hammer just proximal to the olecranon.[14]
Triceps tendinitis can occur with an overload of the muscle. It commonly manifests as chronic posterior elbow pain that worsens with active extension. The condition is commonly seen in men aged 30 to 40 years who are throwing athletes. The typical management strategy for this condition is rest and pain control.
Ruptures of the triceps muscle are rare and typically only occur in anabolic steroid users. Distal triceps ruptures are also relatively uncommon. The reason they are not common revolves primarily around the anatomy of the triceps muscle. If a rupture were to occur, it would occur at the tendon-bone junction, resulting from an eccentric contraction of the muscle. The injury typically occurs due to either a fall on an outstretched hand or a direct blow to the triceps tendon. The patient presents after a painful popping sensation with pain and swelling over the posterior elbow with the inability to extend the elbow against resistance. Surgical consideration for a partial rupture is controversial, but it is necessary for a complete rupture. If the rupture is chronic, then along with surgical repair, remodeling is also indicated.[15]
Other Issues
The triceps brachii can undergo training in a variety of different ways. It can be worked out in isolation or with compound elbow extension movements. It can also be contracted statically to keep the arm straight against resistance.[16]
Examples of isolation movements include lying triceps extensions, behind-the-back arm extensions, cable push-downs, and standing triceps "kickbacks." The compound exercises that work out the triceps include any pressing movements like push-ups, bench presses, close grip bench presses, tricep dips, and military presses.[17] The closer the grip on these exercises, the more the movement will isolate the triceps. The wider the grip, the more they work the outer chest.
Static contraction movements include pullovers, straight-arm pull-downs, and bent-over lateral raises, which are also used to build the deltoids and latissimus dorsi.
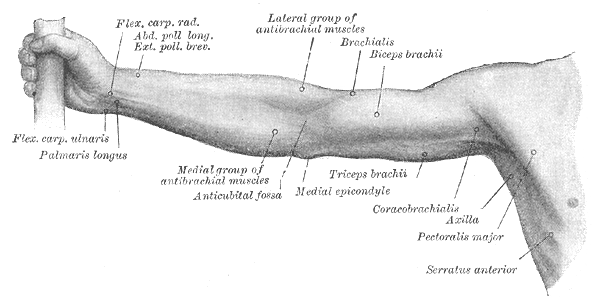
(Click Image to Enlarge)
Right Upper Extremity Surface Anatomy. This anterior view shows the surface markings of the flexor carpi radialis, abductor and exterior pollicis longus and brevis, palmaris longus, medial antebrachial muscles, antecubital fossa, lateral antebrachial muscles, brachialis, biceps brachii, triceps brachii, and medial epicondyle.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
<p>Contributed by RS Menon, MD (https://www.youtube.com/watch?v=62jADalpDaI)</p>
Madsen M, Marx RG, Millett PJ, Rodeo SA, Sperling JW, Warren RF. Surgical anatomy of the triceps brachii tendon: anatomical study and clinical correlation. The American journal of sports medicine. 2006 Nov:34(11):1839-43
[PubMed PMID: 16735585]
Kholinne E, Zulkarnain RF, Sun YC, Lim S, Chun JM, Jeon IH. The different role of each head of the triceps brachii muscle in elbow extension. Acta orthopaedica et traumatologica turcica. 2018 May:52(3):201-205. doi: 10.1016/j.aott.2018.02.005. Epub 2018 Mar 2
[PubMed PMID: 29503079]
Jenkins S, Bordes S, Olewnik Ł, Haładaj R, Iwanaga J, Loukas M, Dumont AS, Bui CJ, Tubbs RS. The proximal humeral attachment of the lateral head of the triceps brachii: a cadaveric study and potential site for radial nerve compression. Acta neurochirurgica. 2021 Mar:163(3):615-618. doi: 10.1007/s00701-020-04527-y. Epub 2020 Aug 13
[PubMed PMID: 32789596]
Grzonkowska M, Badura M, Lisiecki J, Szpinda M, Baumgart M, Wiśniewski M. Growth dynamics of the triceps brachii muscle in the human fetus. Advances in clinical and experimental medicine : official organ Wroclaw Medical University. 2014 Mar-Apr:23(2):177-84
[PubMed PMID: 24913107]
Ledro G, Turrina A, Picelli A, Stecco C, Principe F, Cacciatori C, Smania N. Brachial artery blood flow during submaximal isometric contraction of the biceps brachii and triceps brachii in humans: a preliminary observation. Journal of bodywork and movement therapies. 2013 Apr:17(2):165-8. doi: 10.1016/j.jbmt.2012.07.014. Epub 2012 Aug 21
[PubMed PMID: 23561862]
Athlani L, Delgove A, Dautel G, Casoli V. Anatomy of the ulnar nerve in the posterior compartment of the upper arm: Relationships with the triceps brachii muscle. Morphologie : bulletin de l'Association des anatomistes. 2020 May:104(345):85-90. doi: 10.1016/j.morpho.2019.11.001. Epub 2020 Apr 15
[PubMed PMID: 32305208]
Erhardt AJ, Futterman B. Variations in the Innervation of the Long Head of the Triceps Brachii: A Cadaveric Investigation. Clinical orthopaedics and related research. 2017 Jan:475(1):247-250. doi: 10.1007/s11999-016-5146-z. Epub 2016 Nov 9
[PubMed PMID: 27830483]
Rezzouk J, Durandeau A, Vital JM, Fabre T. [Long head of the triceps brachii in axillary nerve injury: anatomy and clinical aspects]. Revue de chirurgie orthopedique et reparatrice de l'appareil moteur. 2002 Oct:88(6):561-4
[PubMed PMID: 12447125]
Villani F, Piquilloud G, Casoli V. The medial head of triceps brachii: a muscular flap. Journal of plastic, reconstructive & aesthetic surgery : JPRAS. 2012 Sep:65(9):e263-4. doi: 10.1016/j.bjps.2012.02.023. Epub 2012 Mar 23
[PubMed PMID: 22445693]
Maeo S, Wu Y, Huang M, Sakurai H, Kusagawa Y, Sugiyama T, Kanehisa H, Isaka T. Triceps brachii hypertrophy is substantially greater after elbow extension training performed in the overhead versus neutral arm position. European journal of sport science. 2023 Jul:23(7):1240-1250. doi: 10.1080/17461391.2022.2100279. Epub 2022 Aug 11
[PubMed PMID: 35819335]
Zaras N, Stasinaki AN, Mpampoulis T, Spiliopoulou P, Hadjicharalambous M, Terzis G. Effect of Inter-Repetition Rest Vs. Traditional Resistance Training on The Upper Body Strength Rate of Force Development and Triceps Brachii Muscle Architecture. Journal of human kinetics. 2022 Jan:81():189-198. doi: 10.2478/hukin-2022-0016. Epub 2022 Feb 10
[PubMed PMID: 35291627]
Use the mouse wheel to zoom in and out, click and drag to pan the image