Introduction
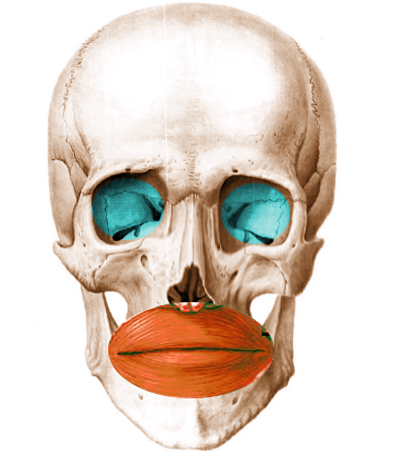
Orbicularis oris muscle, also known as musculus orbicularis oris is a complex, multi-layered muscle which attaches through a thin, superficial musculoaponeurotic system to the dermis of the upper lip and lower lip and serves as an attachment site for many other facial muscles around the oral region.[1] This muscle may be regarded as a single muscle anatomically, but functionally it appears to consist of different parts that act either independently or together with other facial muscles.[2] It has neither a bony or tendinous origin.
Earlier, some authors were of the opinion that this muscle is a sphincter muscle as it encircles the orifice of the mouth. But, this theory was discarded as research found that fibers of this muscle run in different directions rather than running in a uniformly circular manner.
Structure and Function
Orbicularis muscle has a dual function. The deep fiber acts like a constrictor and is responsible for the sphincteric action of the mouth. It is related to holding food due to general sphincteric activity along with other muscular loops of the oropharynx; this is known as the “archaic” part of the muscle.[3] The superficial fiber is the retractor fiber and is related to the facial expression and the precise movements of lips needed in speech.[3]
Orbicularis oris, function in association with the cheek muscles to create contact between the teeth and lips by pressurizing the dental arches[4] and collaborating in the production of speech sounds.[4][5] It is also crucial for swallowing, mastication, and sucking.[6][7]
This muscle also helps in puckering the lips due to which it is sometimes known as the “kissing muscle.” The musicians also use this muscle when they play brass or woodwind instruments.
Embryology
The muscle is a derivative of the mesoderm of the second branchial arch.[8] Between the 3rd and 8th week, mesoderm of the second arch starts thickening. Between 6 and 8 weeks, premyloblasts and myeloblasts which appear as sheet-like collection begin to extend to form five different laminae.[8] The orbicularis oris muscle develops from two embryonic laminae, the mandibular lamina (which differentiates partially into the lower fibers of the muscle) and the infraorbital lamina (which develops into the upper fibers of the muscle).[9]
Blood Supply and Lymphatics
The main blood supply of this muscle is from the facial artery. Two of the branches of this artery, namely the superior labial branch and inferior labial branch, supply the muscle. It also receives supply from the maxillary artery via mental and infra-orbital branch. Superficial temporal artery via its transverse facial branch also supplies this muscle.
Nerves
Within the parotid gland, the facial nerve divides into five motor branches. Orbicularis oris muscle receives nerve supply from the buccal and mandibular branches of the facial nerve (derived from the second pharyngeal arch).[10]
Muscles
The orbicularis muscle consists of two well-defined parts, namely a deep and a superficial part. These two parts have different names from different authors, such as[11]
- Deep part and superficial part
- Pars marginalis and pars superficialis
- Marginal part and peripheral part
- Intrinsic and extrinsic bundle
The deep fibers of the orbicularis oris muscle originate from the modiolus on each side. These fibers run horizontal passing from one commissure of the oral cavity to the other across the midline and lie close to the inner mucosal surface.[3] The lower border of these fibers curls upon themselves, forming the vermilion by everting the mucous membrane.
The superficial orbicularis oris muscle fiber originates from the muscles of facial expression. The superficial muscle fiber divides into an upper and lower bundle. The lower bundle, also known as the nasolabial bundle receives fibers from the depressor anguli oris muscle on each side. They insert in the skin forming the ridges at philtrum with short fibers ending in the ipsilateral ridge and long fibers crossing the midline to insert into the contralateral one.[3] The upper bundle also is known as the nasal bundle represents the common insertion of the fibers of various muscles such as the zygomaticus major and minor, levator labii superioris, levator labii superioris alaeque nasi and transversus nasi. They insert into the anterior nasal spine, the septo-premaxillary ligament, and the nostril sill, passing deep to the alar base.[3]
Physiologic Variants
Some newborns may be born with an absence of the orbicularis oris on one side of the face, which results in a partial droop on the affected side.
Surgical Considerations
Tension on this muscle results in smoker’s line or vertical lip line/rhytids on upper as well as the lower lip. Treatment of these lines consists of botulinum toxin injected directly into the muscle.[12]
Contraction of this muscle results in marionette lines in lateral perioral region. These lines give the illusion of sadness. Treatment of these lines is similar to the treatment of smoker’s line.[12]
In cleft lip: Orbicularis oris muscle is the most critical structure affected in the cleft lip as it is responsible for various movements of the orofacial region and also contributes to the contour of the lip region. Its proper orientation is crucial for its normal function. During reconstruction surgery in cleft lip cases, restoration of anatomical and functional components of the upper lip is the prime objective for which it is imperative to re-establish the normal course of this muscle.[3]
Clinical Significance
In facial palsy: As the muscle receives nerve supply from the seventh cranial nerve, thus, injury to this nerve can result in paralysis of the muscle. In Bell palsy, sagging of the orbicularis oris results in drooling.[12]
Loss of tone: Loss of tone of this muscle to the muscles leads to drooping of the commissure as it controls the oral sphincter, which can cause drooling and difficulty in eating.[13]
Clinical implication in prosthodontics: The orbicularis oris muscle due to its fiber orientation has a positive action in maintaining the stability of the denture. Placing the artificial teeth so as not to interfere with muscle activity and to enable the retention and stability action of the musculature is a priority of the treatment in complete denture cases.[14][15]
In the oral cavity, the peri-oral muscles, mainly the orbicularis oris and the buccinator, exert inward forces. Balancing these forces are the outward forces exerted by the tongue. The impression for complete denture must be molded by muscle function so that it is in harmony with these surrounding structures.[16]
As orbicularis oris is the main muscle of the lip, its tone depends on the support it receives from labial flange that lies in the labial vestibule (extending from buccal frenum in the canine region on one side to the other side) and position of teeth.[17] Thus, this muscle influences the thickness of the flange. When the mouth is open wide, the muscle becomes stretched, thereby, narrowing the sulcus. If the flanges are thick, it will displace the denture.[17]
If the teeth position is too far labially, the orbicularis oris gets stretched. This stretching effect of the lips against the teeth also tends to exert a dislodging force on the maxillary denture.[17]
Orbicularis oris muscle along with the buccinator and pharyngeal constrictor form a functional unit, known as "buccinator mechanism" which has an important role in orofacial function (swallowing, sucking, whistling, chewing, vowel pronunciation, kissing).[17] If buccinator and orbicularis oris muscles are weakened or paralyzed, food tends to accumulate in the oral vestibule during chewing.
Other Issues
Percussion on the lateral aspect of the nose or the upper lip of the infants results in elevation of the oral commissure on the ipsilateral side. This maneuver is referred to as orbicularis oris reflex (snout reflex). This reflex disappears itself during the later stages of life.[18]