[1]
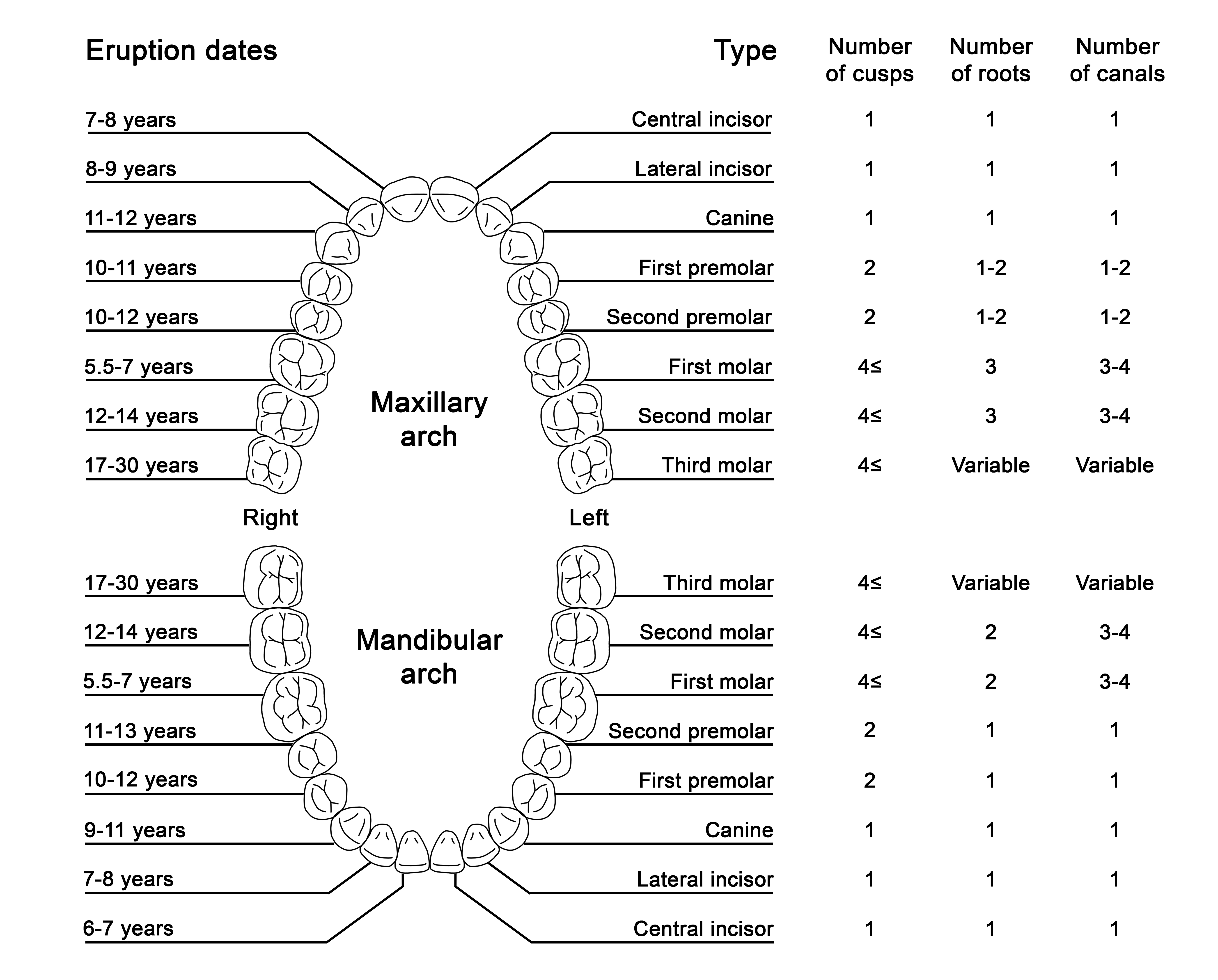
ADA Division of Communications, Journal of the American Dental Association, ADA Council on Scientific Affairs. For the dental patient. Tooth eruption: the permanent teeth. Journal of the American Dental Association (1939). 2006 Jan:137(1):127
[PubMed PMID: 16457009]
[2]
Koussoulakou DS, Margaritis LH, Koussoulakos SL. A curriculum vitae of teeth: evolution, generation, regeneration. International journal of biological sciences. 2009:5(3):226-43
[PubMed PMID: 19266065]
[3]
Al-Jawad M, Steuwer A, Kilcoyne SH, Shore RC, Cywinski R, Wood DJ. 2D mapping of texture and lattice parameters of dental enamel. Biomaterials. 2007 Jun:28(18):2908-14
[PubMed PMID: 17367851]
[4]
Beniash E, Stifler CA, Sun CY, Jung GS, Qin Z, Buehler MJ, Gilbert PUPA. The hidden structure of human enamel. Nature communications. 2019 Sep 26:10(1):4383. doi: 10.1038/s41467-019-12185-7. Epub 2019 Sep 26
[PubMed PMID: 31558712]
Level 2 (mid-level) evidence
[5]
Arola DD, Gao S, Zhang H, Masri R. The Tooth: Its Structure and Properties. Dental clinics of North America. 2017 Oct:61(4):651-668. doi: 10.1016/j.cden.2017.05.001. Epub
[PubMed PMID: 28886762]
[6]
Goldberg M, Kulkarni AB, Young M, Boskey A. Dentin: structure, composition and mineralization. Frontiers in bioscience (Elite edition). 2011 Jan 1:3(2):711-35
[PubMed PMID: 21196346]
[7]
Ivancik J, Arola DD. The importance of microstructural variations on the fracture toughness of human dentin. Biomaterials. 2013 Jan:34(4):864-74. doi: 10.1016/j.biomaterials.2012.10.032. Epub 2012 Nov 3
[PubMed PMID: 23131531]
[8]
Yu C, Abbott PV. An overview of the dental pulp: its functions and responses to injury. Australian dental journal. 2007 Mar:52(1 Suppl):S4-16
[PubMed PMID: 17546858]
Level 3 (low-level) evidence
[9]
Zanini M, Meyer E, Simon S. Pulp Inflammation Diagnosis from Clinical to Inflammatory Mediators: A Systematic Review. Journal of endodontics. 2017 Jul:43(7):1033-1051. doi: 10.1016/j.joen.2017.02.009. Epub 2017 May 17
[PubMed PMID: 28527838]
Level 1 (high-level) evidence
[10]
Nanci A, Bosshardt DD. Structure of periodontal tissues in health and disease. Periodontology 2000. 2006:40():11-28
[PubMed PMID: 16398683]
[11]
Yumoto H, Hirao K, Hosokawa Y, Kuramoto H, Takegawa D, Nakanishi T, Matsuo T. The roles of odontoblasts in dental pulp innate immunity. The Japanese dental science review. 2018 Aug:54(3):105-117. doi: 10.1016/j.jdsr.2018.03.001. Epub 2018 Mar 27
[PubMed PMID: 30128058]
[12]
Farges JC, Alliot-Licht B, Renard E, Ducret M, Gaudin A, Smith AJ, Cooper PR. Dental Pulp Defence and Repair Mechanisms in Dental Caries. Mediators of inflammation. 2015:2015():230251. doi: 10.1155/2015/230251. Epub 2015 Oct 11
[PubMed PMID: 26538821]
[13]
Yamamoto T, Hasegawa T, Yamamoto T, Hongo H, Amizuka N. Histology of human cementum: Its structure, function, and development. The Japanese dental science review. 2016 Aug:52(3):63-74. doi: 10.1016/j.jdsr.2016.04.002. Epub 2016 Apr 27
[PubMed PMID: 28408958]
[14]
Miletich I, Sharpe PT. Neural crest contribution to mammalian tooth formation. Birth defects research. Part C, Embryo today : reviews. 2004 Jun:72(2):200-12
[PubMed PMID: 15269893]
[15]
Hovorakova M, Lesot H, Peterka M, Peterkova R. The developmental relationship between the deciduous dentition and the oral vestibule in human embryos. Anatomy and embryology. 2005 Apr:209(4):303-13
[PubMed PMID: 15666156]
[16]
Zou D, Zhao J, Ding W, Xia L, Jang X, Huang Y. Wisdom teeth: mankind's future third vice-teeth? Medical hypotheses. 2010 Jan:74(1):52-5. doi: 10.1016/j.mehy.2009.08.004. Epub 2009 Sep 17
[PubMed PMID: 19765911]
[18]
Maia FPA, de Sousa Filho GC, Pacífico FA, Albuquerque LCA, de Melo Vasconcelos AF, do Egito Vasconcelos BC. Proximity of the maxillary artery to the neck of the mandibular condyle: anatomical study. Oral and maxillofacial surgery. 2019 Dec:23(4):423-427. doi: 10.1007/s10006-019-00788-9. Epub 2019 Jul 5
[PubMed PMID: 31278592]
[20]
Claire PG, Gibbs K, Hwang SH, Hill RV. Divided and reunited maxillary artery: developmental and clinical considerations. Anatomical science international. 2011 Dec:86(4):232-6. doi: 10.1007/s12565-011-0106-x. Epub 2011 Apr 19
[PubMed PMID: 21503610]
[21]
Jergenson MA, Norton NS, Opack JM, Barritt LC. Unique origin of the inferior alveolar artery. Clinical anatomy (New York, N.Y.). 2005 Nov:18(8):597-601
[PubMed PMID: 16187317]
[22]
Oehmke MJ, Knolle E, Oehmke HJ. Lymph drainage in the human dental pulp. Microscopy research and technique. 2003 Oct 15:62(3):187-91
[PubMed PMID: 14506683]
[23]
Amodini Rajakaruna G, Umeda M, Uchida K, Furukawa A, Yuan B, Suzuki Y, Noriko E, Izumi Y, Eishi Y. Possible translocation of periodontal pathogens into the lymph nodes draining the oral cavity. Journal of microbiology (Seoul, Korea). 2012 Oct:50(5):827-36. doi: 10.1007/s12275-012-2030-8. Epub 2012 Nov 4
[PubMed PMID: 23124752]
[24]
Rodella LF, Buffoli B, Labanca M, Rezzani R. A review of the mandibular and maxillary nerve supplies and their clinical relevance. Archives of oral biology. 2012 Apr:57(4):323-34. doi: 10.1016/j.archoralbio.2011.09.007. Epub 2011 Oct 11
[PubMed PMID: 21996489]
[26]
Mavrodisz K, Rózsa N, Budai M, Soós A, Pap I, Tarján I. Prevalence of accessory tooth cusps in a contemporary and ancestral Hungarian population. European journal of orthodontics. 2007 Apr:29(2):166-9
[PubMed PMID: 17317866]
[27]
Canoglu E, Canoglu H, Aktas A, Cehreli ZC. Isolated bilateral macrodontia of mandibular second premolars: A case report. European journal of dentistry. 2012 Jul:6(3):330-4
[PubMed PMID: 22904663]
Level 3 (low-level) evidence
[28]
Chen Y, Zhou F, Peng Y, Chen L, Wang Y. Non-syndromic occurrence of true generalized microdontia with hypodontia: A case report. Medicine. 2019 Jun:98(26):e16283. doi: 10.1097/MD.0000000000016283. Epub
[PubMed PMID: 31261601]
Level 3 (low-level) evidence
[29]
Jayashankara C, Shivanna AK, Sridhara K, Kumar PS. Taurodontism: A dental rarity. Journal of oral and maxillofacial pathology : JOMFP. 2013 Sep:17(3):478. doi: 10.4103/0973-029X.125227. Epub
[PubMed PMID: 24574680]
[30]
Sharada HL, Deo B, Briget B. Gemination of a permanent lateral incisor- a case report with special emphasis on management. Journal of international oral health : JIOH. 2013 Apr:5(2):49-53
[PubMed PMID: 24155591]
Level 3 (low-level) evidence
[31]
Ley AM, Viana FLP, Cruz SML, Vasconcelos BC. Fused tooth: clinical approach to endodontic treatment. General dentistry. 2019 Nov-Dec:67(6):59-61
[PubMed PMID: 31658027]
[32]
Palermo D, Davies-House A. Unusual finding of concrescence. BMJ case reports. 2016 Mar 23:2016():. doi: 10.1136/bcr-2016-214597. Epub 2016 Mar 23
[PubMed PMID: 27009195]
Level 3 (low-level) evidence
[33]
Meighani G, Pakdaman A. Diagnosis and management of supernumerary (mesiodens): a review of the literature. Journal of dentistry (Tehran, Iran). 2010 Winter:7(1):41-9
[PubMed PMID: 21998774]
[34]
Demiriz L, Durmuşlar MC, Mısır AF. Prevalence and characteristics of supernumerary teeth: A survey on 7348 people. Journal of International Society of Preventive & Community Dentistry. 2015 May:5(Suppl 1):S39-43. doi: 10.4103/2231-0762.156151. Epub
[PubMed PMID: 25984466]
Level 3 (low-level) evidence
[35]
Ata-Ali F, Ata-Ali J, Peñarrocha-Oltra D, Peñarrocha-Diago M. Prevalence, etiology, diagnosis, treatment and complications of supernumerary teeth. Journal of clinical and experimental dentistry. 2014 Oct:6(4):e414-8. doi: 10.4317/jced.51499. Epub 2014 Oct 1
[PubMed PMID: 25593666]
[36]
Bala M, Pathak A. Ectodermal dysplasia with true anodontia. Journal of oral and maxillofacial pathology : JOMFP. 2011 May:15(2):244-6. doi: 10.4103/0973-029X.84515. Epub
[PubMed PMID: 22529591]
[37]
Jonsson L, Magnusson TE, Thordarson A, Jonsson T, Geller F, Feenstra B, Melbye M, Nohr EA, Vucic S, Dhamo B, Rivadeneira F, Ongkosuwito EM, Wolvius EB, Leslie EJ, Marazita ML, Howe BJ, Moreno Uribe LM, Alonso I, Santos M, Pinho T, Jonsson R, Audolfsson G, Gudmundsson L, Nawaz MS, Olafsson S, Gustafsson O, Ingason A, Unnsteinsdottir U, Bjornsdottir G, Walters GB, Zervas M, Oddsson A, Gudbjartsson DF, Steinberg S, Stefansson H, Stefansson K. Rare and Common Variants Conferring Risk of Tooth Agenesis. Journal of dental research. 2018 May:97(5):515-522. doi: 10.1177/0022034517750109. Epub 2018 Jan 24
[PubMed PMID: 29364747]
[38]
Rakhshan V. Congenitally missing teeth (hypodontia): A review of the literature concerning the etiology, prevalence, risk factors, patterns and treatment. Dental research journal. 2015 Jan-Feb:12(1):1-13
[PubMed PMID: 25709668]
[39]
Bural C, Oztas E, Ozturk S, Bayraktar G. Multidisciplinary treatment of non-syndromic oligodontia. European journal of dentistry. 2012 Apr:6(2):218-26
[PubMed PMID: 22509127]
[40]
Sarikov R, Juodzbalys G. Inferior alveolar nerve injury after mandibular third molar extraction: a literature review. Journal of oral & maxillofacial research. 2014 Oct-Dec:5(4):e1. doi: 10.5037/jomr.2014.5401. Epub 2014 Dec 29
[PubMed PMID: 25635208]
[41]
Leung YY. Management and prevention of third molar surgery-related trigeminal nerve injury: time for a rethink. Journal of the Korean Association of Oral and Maxillofacial Surgeons. 2019 Oct:45(5):233-240. doi: 10.5125/jkaoms.2019.45.5.233. Epub 2019 Oct 30
[PubMed PMID: 31728330]
[42]
Saha N, Kedarnath NS, Singh M. Orthopantomography and Cone-Beam Computed Tomography for the Relation of Inferior Alveolar Nerve to the Impacted Mandibular Third Molars. Annals of maxillofacial surgery. 2019 Jan-Jun:9(1):4-9. doi: 10.4103/ams.ams_138_18. Epub
[PubMed PMID: 31293923]
[43]
Pitros P, O'Connor N, Tryfonos A, Lopes V. A systematic review of the complications of high-risk third molar removal and coronectomy: development of a decision tree model and preliminary health economic analysis to assist in treatment planning. The British journal of oral & maxillofacial surgery. 2020 Nov:58(9):e16-e24. doi: 10.1016/j.bjoms.2020.07.015. Epub 2020 Aug 14
[PubMed PMID: 32800608]
Level 1 (high-level) evidence
[44]
Khandelwal P, Hajira N. Management of Oro-antral Communication and Fistula: Various Surgical Options. World journal of plastic surgery. 2017 Jan:6(1):3-8
[PubMed PMID: 28289607]
[45]
Nayyar J, Clarke M, O'Sullivan M, Stassen LF. Fractured root tips during dental extractions and retained root fragments. A clinical dilemma? British dental journal. 2015 Mar 13:218(5):285-90. doi: 10.1038/sj.bdj.2015.147. Epub
[PubMed PMID: 25766165]
[46]
Zairi A, Lambrianidis T. Accidental extrusion of sodium hypochlorite into the maxillary sinus. Quintessence international (Berlin, Germany : 1985). 2008 Oct:39(9):745-8
[PubMed PMID: 19093046]
[47]
Wali R, Halai T, Koshal S. WHO surgical safety checklist training: An alternative approach to training in local safety standards for invasive procedures. European journal of dental education : official journal of the Association for Dental Education in Europe. 2020 Feb:24(1):71-78. doi: 10.1111/eje.12469. Epub 2019 Sep 29
[PubMed PMID: 31518469]
[48]
Jan AM, Albenayan R, Alsharkawi D, Jadu FM. The prevalence and causes of wrong tooth extraction. Nigerian journal of clinical practice. 2019 Dec:22(12):1706-1714. doi: 10.4103/njcp.njcp_206_19. Epub
[PubMed PMID: 31793478]