Introduction
The hand serves as the origin and/or insertion for a vast number of muscles. The intrinsic muscles of the hand contain the origin and insertions within the carpal and metacarpal bones. The extrinsic muscles of the hand originate outside the hand, commonly the forearm, and insert into hand structures. A rule of thumb is that any muscle tendon that crosses a joint will act on that joint. For example, muscles of the forearm that cross the carpometacarpal joint will produce flexion or extension at the wrist joint.
Structure and Function
Intrinsic hand muscles originate and insert from the bones, ligaments, and fascia of the hand. These muscles primarily produce fine motor movements. These muscles are divided into thenar, hypothenar, and adductor compartments.[1]
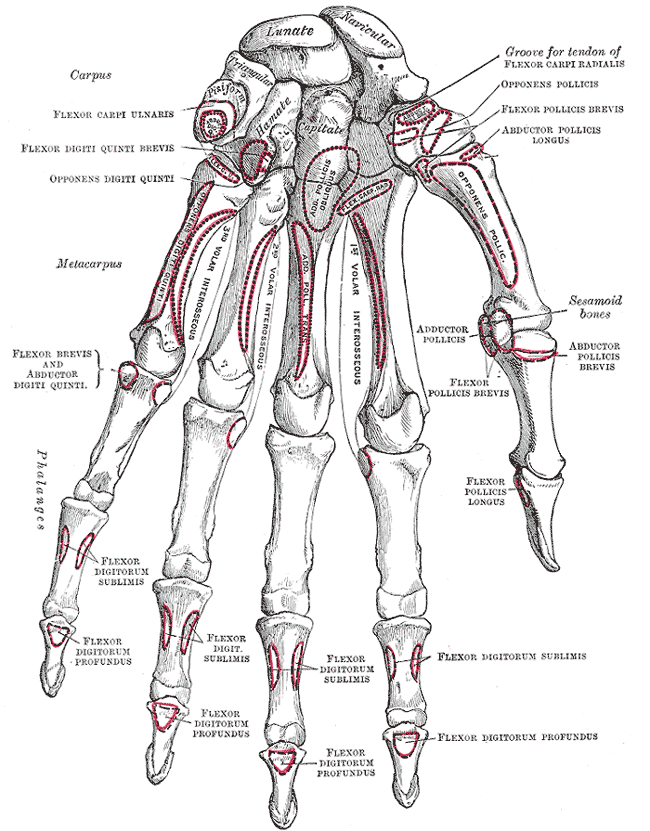
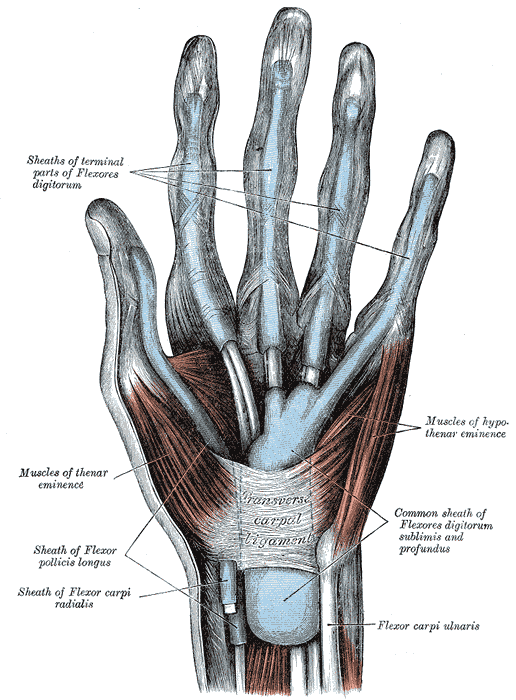
The thenar muscles are a group of three muscles that act on the thumb. These muscles form the bulge on the palmar surface of the thumb and palm, called the thenar eminence. The largest of the three muscles, opponens pollicis, originates at the tubercle of the trapezium and inserts at the lateral margin of the metacarpal of the thumb. It permits the thumb to perform opposition which is the motion of reaching across the palm towards the little finger, by flexing and medially rotating the metacarpal on the axis of the trapezium. The abductor pollicis brevis muscle is positioned anterior to the opponens pollicis and is the primary muscle providing the act of opposition. It originates at the tubercles of the scaphoid and trapezium and inserts at the lateral aspect of the proximal phalanx of the thumb. Abductor pollicis brevis also acts by drawing the thumb away from the midline, which is the action of abduction for all muscles. The flexor pollicis brevis originates at the tubercle of the trapezium via the deep head, and the associated flexor retinaculum via the superficial head, and inserts at the base of the proximal phalanx of the thumb. These three muscles are all innervated by the recurrent branch of the median nerve. The flexor pollicis brevis receives dual innervation with fibers from both the median and ulnar nerves. The superficial head is innervated by the median nerve while the deep head is innervated by the ulnar nerve.
The hypothenar muscles act on the little finger and form a bulge on the medial palmar surface, called the hypothenar eminence, which is less prominent then the thenar eminence. The opponens digiti minimi originates at the hook of hamate and associated transverse carpal ligament and inserts at the ulnar side of the fifth metacarpal. Contraction of the opponens digiti minimi draws the small finger radially, reaching across the palm by flexion and supination, thus performing opposition. The action of the opponens pollicis and opponens digiti minimi allow for the thumb and the little finger to touch. Abductor digiti minimi originates from the pisiform bone and the tendon of flexor carpi ulnaris and inserts at the ulnar base of the proximal phalanx of the small finger. Contraction of this muscle allows for abduction, just as the abductor pollicis brevis muscle directs the thumb away from the midline. Flexor digiti minimi brevis originates at the hook of hamate and the transverse carpal ligament and inserts at the base of the proximal phalanx of the small finger. Palmaris brevis originates at the transverse carpal ligament and inserts on the skin of the medial palm. It permits the wrinkling of the skin on the palmar surface of the hand and protects the ulnar nerve. The ulnar nerve innervates all muscles of the hypothenar compartment.
The adductor pollicis muscle occupies the adductor compartment. The adductor pollicis muscle originates from two places, the oblique and transverse heads. The oblique head originates at the capitate, second and third metacarpals, and inserts at the ulnar base of the proximal phalanx of the thumb. The transverse head arises at the third metacarpal and also inserts at the medial aspect of the proximal phalanx of the thumb. The ulnar nerve provides innervation. This muscle allows for the adduction and flexion of the metacarpophalangeal joint.[2]
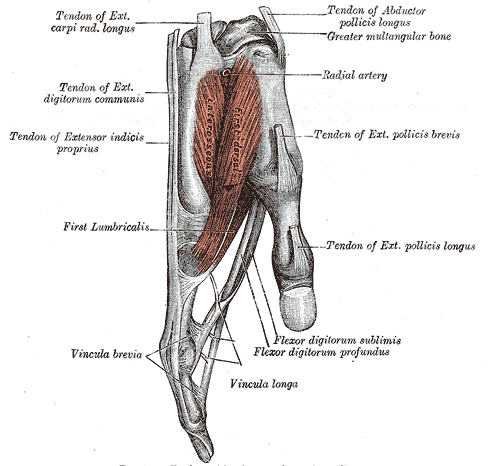
If you make the shape of an L by straightening your second through fifth fingers, via the extension at the proximal interphalangeal joints, and flexion at the metacarpophalangeal joints, you are using muscles of the hand called lumbricals.[3] There are four lumbricals. The first two lumbricals originate from the radial aspect of the first and second tendons of flexor digitorum profundus and insert at the radial lateral bands. The median nerve provides innervation to the two radial lumbricals. The third and fourth lumbricals originate from the ulnar aspect of the medial three flexor digitorum profundus tendons and insert at the radial lateral bands. The ulnar nerve innervates the two ulnar lumbricals. The first and second lumbricals are unipennate, meaning that all muscle fascicles positioned on the same side of a particular tendon. The third and fourth lumbricals are bipennate, meaning run on both sides of the ligament and are innervated by the median nerve.
The interossei muscles act by adducting and abducting the fingers. The mnemonic PAD and DAB helps to remember the actions of each muscle. The "P" in PAD stands for the palmar interossei. Interossei muscles on the palmar surface adduct the fingers, bringing them towards the midline. The "D" in DAB stands for dorsal interossei. The dorsally placed interossei permit abduction of the phalanges, moving them away from the midline. The second and third letters of PAD and DAB stand for the direction of finger movement. The dorsal interossei originate from the adjacent sides of two metacarpals. They insert at the extensor hood and proximal phalanx of each phalange. There are three palmar interossei, which each originate at the medial or lateral surface of the 2nd, 4th, and 5th metacarpals and insert at the base of digits 2-4 and the extensor hood of each finger.[4] These muscles receive innervation from the deep branch of the ulnar nerve. The dorsal interossei are bipennate, and the palmar interossei are unipennate.
The extrinsic muscles of the hand originate in the forearm and are located on the anterior and posterior aspect of the forearm, with flexors positioned anteriorly and extensors posteriorly. These muscles perform the gross movements of the hand and wrist.
The extrinsic muscles of the hand are defined by a proximal origin with an insertion on the hand. The muscles can be grouped by anatomy and function. The muscles included in the anterior forearm with insertion on the hand can be further divided into superficial, intermediate, and deep groups. The majority of the muscles in the group are flexor muscles. The superficial group includes the flexor carpi radialis, palmaris longus, and flexor carpi ulnaris. The flexor carpi ulnaris is innervated by the ulnar nerve while both the flexor carpi radialis and palmaris longus are innervated by the median nerve. Each of these muscles allows for the flexion of the wrist. The flexor carpi ulnaris aids in the ulnar deviation of the hand and is opposed by the flexor carpi radialis that allows for the radial deviation of the hand. The intermediate group includes the flexor digitorum superficialis. This muscle is innervated by the median nerve and allows for flexion of the wrist, MCP, and PIP joints of digits 2-5. The deep group includes the flexor digitorum profundus and flexor pollicis longus. The flexor digitorum profundus has a mixed innervation. The 2nd and 3rd digits receive innervation from the median nerve while the 4th and 5th digits receive innervation from the ulnar nerve. The muscles flex the DIP joints for digits 2-5. The flexor pollicis longus is innervated by the median nerve and flexes the wrist, MCP, and IP joint of the thumb.
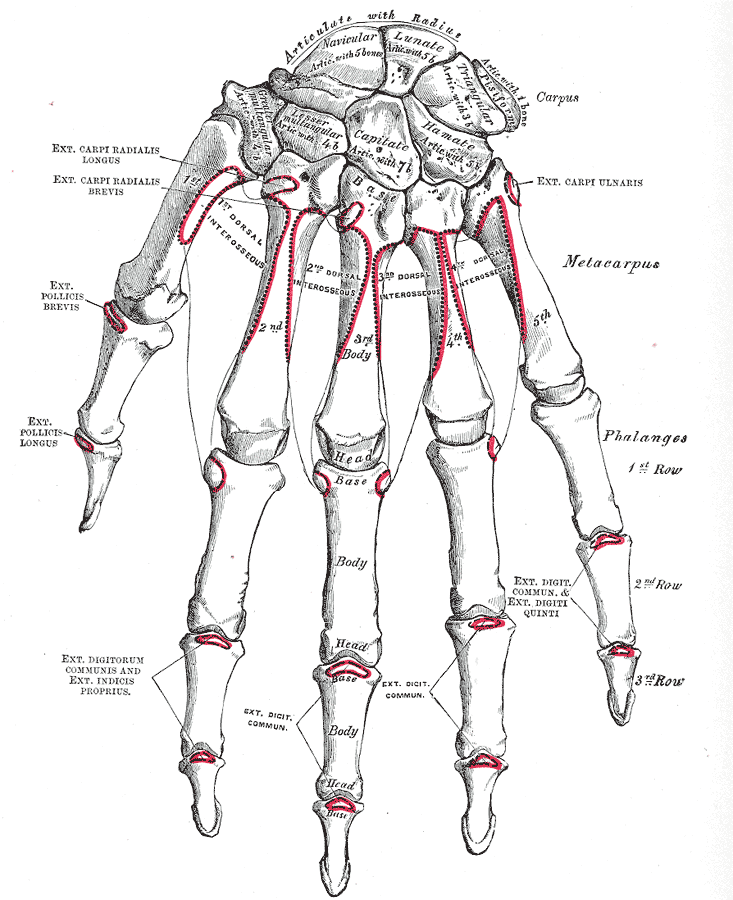
The posterior forearm is divided into superficial and deep muscle layers. The majority of muscles in the group are extensor muscles. The superficial layers include the extensor carpi radialis longus, extensor carpi radialis brevis, extensor digitorum, extensor digiti minimi, and extensor carpi ulnaris. This group of muscles aid in the extension of the wrist; extension of the MCP, and IP joint of digits; and adduction and abduction of the wrist. The deep group includes the abductor pollicis longus, extensor pollicis longus, extensor pollicis brevis, and extensor indicis. This group of muscles aid in the extension of the wrist; abduction and extension of thumb; and extension of the 2nd digit.
Embryology
The development of the hand occurs between 6-14 weeks of gestation and is separated into three phases. The first stage occurs between 6-10 weeks. During this phase, the initial shape of the hand can be appreciated. The second phase occurs between 10-13 weeks and is characterized by the appearance of creases in the hand. Finally during the last phase which begins at 13 weeks, the hand ridges are created. [5]
Blood Supply and Lymphatics
The primary blood supply of the hand comes from the deep palmar and superficial palmar arches. The superficial branch of the radial artery forms anastomoses with the superficial palmar arch. The deep branch of the radial artery runs through the dorsal interossei muscle and anastomoses at the deep palmar arch. The ulnar artery divides into a deep branch which anastomoses with the deep palmar arch, and a superficial branch which ends at the superficial palmar arch. This anastomosing network allows for blood supply coming from multiple directions allowing for vast collateral blood supply to prevent ischemic injury
The lymphatic system creates a pathway for lymphatic drainage from the distal fingertips to the lymph nodes found in the lateral axilla. The pathway originates from capillaries in the fingertip and palms. The lymphatic vessels then travel on the dorsal aspect of the hand. The lymph vessels are found just posterior to the cutaneous veins. The lymph pathway continues up the arm and runs parallel to the basilic vein until the lymphatic system connects to the lymph nodes in the lateral axillary region. The hand is a common site for lymphedema to occur which can hinder the function of the hand muscles described in this article. [6]
Nerves
The innervation of the muscles of the hand is by the ulnar, median, and radial nerves. The ulnar nerve arises from the medial cord of the brachial plexus. The nerve originates from the ventral rami of the C8 and T1 nerve roots. The median nerve arises from the convergence of the lateral and medial cords of the brachial plexus. The nerve originates from the ventral rami of the C5 through T1 nerve root. The radial nerve originates from the ventral rami of the C5 through T1 nerve root and is a terminal branch of the posterior cord.[7][8]
Muscles
Intrinisic Hand Muscles
Thenar Muscles [9]
Abductor pollicis brevis
- Origin: trapezium, scaphoid
- Insertion: lateral base thumb, proximal phalanx
- Action: abduction and opposition of the thumb
- Innervation: median nerve
Opponens pollicis
- Origin: trapezium
- Insertion: first metacarpal
- Action: pronation of the thumb
- Innervation: median nerve
Flexor pollicis brevis
- Origin: superficial head: trapezium and carpal ligament; deep head: second metacarpal
- Insertion: thumb proximal phalanx
- Action: flexion of MCP joint of the thumb
- Innervation: superficial head: median nerve; deep head: ulnar nerve
Hypothenar Muscles [10][11]
Abductor digiti minimi
- Origin: pisiform
- Insertion: proximal phalanx of the fifth digit
- Action: abduction of the fifth digit
- Innervation: ulnar nerve
Flexor digiti minimi brevis
- Origin: hamate and flexor retinaculum
- Insertion: proximal phalanx of the fifth digit
- Action: flexion of the fifth digit
- Innervation: ulnar nerve
Opponens digiti minimi
- Origin: flexor retinaculum
- Insertion: 5th metacarpal
- Action: opposition of the fifth digit
- Innervation: ulnar nerve
Palmaris brevis
- Origin: palmar aponeurosis and flexor retinaculum
- Insertion: skin of hand
- Action: wrinkles the skin, palmar grip
- Innervation: ulnar nerve
Adductor Muscles
Adductor pollicis
- Origin: oblique head: capitate, second, or third metacarpal; transverse head: third metacarpal
- Insertion: thumb proximal phalanx
- Action: adduction of thumb
- Innervation: ulnar nerve
Interossei Muscles [11]
Dorsal Interossei
- Origin: metacarpals
- Insertion: extensor hood and proximal phalanges
- Action: abduction of digits
- Innervation: ulnar nerve
Palmar Interossei
- Origin: metacarpals
- Insertion: extensor hood and proximal phalanges
- Action: adduction of digits
- Innervation: ulnar nerve
Lumbricals [12]
- Origin: tendons of flexor digitorum profundus
- Insertion: extensor hoods of digits
- Action: flexion at MCP joint and extension of IP joints of digits
- Innervation: first and second: median nerve; third and fourth: ulnar nerve
Extrinsic Hand Muscles
Flexor Muscles: Superficial Group [13]
Flexor carpi radialis
- Origin: medial epicondyle of humerus
- Insertion: base of 2nd metacarpal
- Action: flexion and abduction of the hand
- Innervation: median nerve
Palmaris longus
- Origin: medial epicondyle of humerus
- Insertion: palmar aponeurosis and flexor retinaculum
- Action: flexion of the hand
- Innervation: median nerve
Flexor carpi ulnaris
- Origin: medial epicondyle of humerus and olecranon
- Insertion: isoform, hook of hamate, 5th metacarpal
- Action: flexion and adduction of the wrist
- Innervation: ulnar nerve
Flexor Muscles: Intermediate Group
Flexor digitorium superficialis
- Origin: medial epicondyle, coronoid process, and radius
- Insertion: middle phalanges of digits
- Action: flexion of wrist and flexion of the MCP and PIP joints of digits
- Innervation: median nerve
Flexor Muscles: Deep Group
Flexor digitorum profundus
- Origin: ulna and interosseous membrane
- Insertion: base of phalanges
- Action: flexion DIP joints of digits
- Innervation: digits 2-3: median nerve; digits 4-5: ulnar nerve
Flexor pollicis longus
- Origin: radius and interosseous membrane
- Insertion: distal phalanx of thumb
- Action: flexion of the wrist and flexion of the MCP and IP joints of the digits
- Innervation: median nerve
Extensor Muscles
Extensor Muscles: Superficial Group
Extensor carpi radialis longus
- Origin: lateral supracondylar ridge of humerus
- Insertion: base of 2nd metacarpal
- Action: extension and abduction of the wrist
- Innervation: radial nerve
Extensor carpi radialis brevis
- Origin: lateral epicondyle of humerus
- Insertion: base of 3rd metacarpal
- Action: extension and abduction of the wrist
- Innervation: radial nerve
Extensor digitorum
- Origin: lateral epicondyle of humerus
- Insertion: extensor hood of digits
- Action: extension of the wrist and extension of the MCP and IP joints of the digits
- Innervation: posterior interosseous nerve
Extensor digiti minimi
- Origin: lateral epicondyle of humerus
- Insertion: extensor hood of 5th digit
- Action: extension of the wrist and extension of MCP and IP of the 5th digit
- Innervation: posterior interosseous
Extensor carpi ulnaris
- Origin: lateral epicondyle of humerus and ulna
- Insertion: base of 5th metacarpal
- Action: extension and adduction of the wrist
- Innervation: posterior interosseous nerve
Extensor Muscles: Deep Group
Abductor pollicis longus
- Origin: ulna, radius, interosseous membrane
- Insertion: 1st metacarpal
- Action: extension of the wrist, abduction of the thumb, and extension of the CMC joint
- Innervation: posterior interosseous nerve
Extensor pollicis brevis
- Origin: radius and interosseous membrane
- Insertion: phalanx of 1st digit
- Action: extension of the wrist, extension of the thumb and the CMC joint
- Innervation: posterior interosseous nerve
Extensor pollicis longus
- Origin: ulna and interosseous membrane
- Insertion: phalanx of first digit
- Action: extension of the wrist and extension thumb at IP, MCP, and CMC joints
- Innervation: posterior interosseous nerve
Extensor indicis
- Origin: ulna
- Insertion: extensor hood of 2nd digit
- Action: extension of the 2nd digit
- Innervation: posterior interosseous nerve
Surgical Considerations
Due to the hand's extensive musculature, tendon transfers are commonly performed to reduce the deficit from nerve damage. Various muscles of the hand receive innervation from different upper extremity nerves including the median, ulnar, and radial nerves. Therefore, the distribution of innervation within the hand can be used advantageously to correct for nerve palsies. Tendon transfers have successfully been used to correct for function in both intrinsic and extrinsic hand muscles. During the transfer, the insertion point of the muscle is detached and mobilized to the desired location. A tendon transfer is typically considered three months after the injury if the muscle has failed to reinnervate.
Radial nerve palsy classically presents with an inability to extend the wrist, extend the fingers at the MCP joint, and abduct the thumb. Median nerve palsy presents with the loss of abduction and opposition of the thumb; sensory loss over the first three digits; and weak forearm pronation. Ulnar nerve palsy presents with sensory loss over the last two digits and weakness of the lumbrical and flexor digitorum profundus.
In radial nerve palsy, examples of potential donor tendons include the extensor digitorum and flexor carpi radialis. Both of these tendons take into account and advantage of different innervations of the muscles, the posterior interosseous nerve, and median nerve, respectfully. [14]
Clinical Significance
The intrinsic muscles of the hand provide the fine motor movements while the extrinsic muscles permit strength. There are several cases where extrinsic muscles and tendon interruption result in hand deformity and malfunction. Situations, where intrinsic hand muscles are solely affected, are less common but are still relevant. Ulnar nerve compression at Guyon's canal can manifest as atrophy and weakness in interosseous muscles, the third and fourth lumbricals, and adductor pollicis. The physical exam will reveal weakness with abduction and adduction of the fingers, flexion at the MCP and extension at the PIP, and adduction and flexion at the MCP of the thumb. Ulnar nerve compression will also affect the hypothenar compartment because most intrinsic hand muscles receive innervation from the ulnar nerve. Median nerve compression at carpal's tunnel will affect the muscles of the thenar compartment. Carpal tunnel syndrome is elicited on physical exam by Tinel's test, where the practitioner taps on the medial aspect of the wrist at the median nerve. Numbness and tingling during this maneuver is a positive sign. A positive Phalen's sign test is also indicative of carpal tunnel syndrome. The patient raises the hands out in front of himself, flexes the wrist and places the dorsal wrists together, while flexed, for about 60 seconds. Numbness and tingling with this maneuver is also a positive sign. Other injuries of note can be of a traumatic nature, lending to lesions at tendon insertion which would alter the mechanics of the intrinsic muscle involved. For example, if blunt trauma struck the insertion of the opponens pollicis muscle, the action of thumb opposition and supination would be significantly altered despite intact innervation.