[1]
Nascimbene A, Angelini P. Superior vena cava thrombosis and paradoxical embolic stroke due to collateral drainage from the brachiocephalic vein to the left atrium. Texas Heart Institute journal. 2011:38(2):170-3
[PubMed PMID: 21494530]
[2]
Piciucchi S, Barone D, Sanna S, Dubini A, Goodman LR, Oboldi D, Bertocco M, Ciccotosto C, Gavelli G, Carloni A, Poletti V. The azygos vein pathway: an overview from anatomical variations to pathological changes. Insights into imaging. 2014 Oct:5(5):619-28. doi: 10.1007/s13244-014-0351-3. Epub 2014 Aug 30
[PubMed PMID: 25171956]
Level 3 (low-level) evidence
[3]
Fell SC. Surgical anatomy of the diaphragm and the phrenic nerve. Chest surgery clinics of North America. 1998 May:8(2):281-94
[PubMed PMID: 9619305]
[4]
Furlow PW, Mathisen DJ. Surgical anatomy of the trachea. Annals of cardiothoracic surgery. 2018 Mar:7(2):255-260. doi: 10.21037/acs.2018.03.01. Epub
[PubMed PMID: 29707503]
[5]
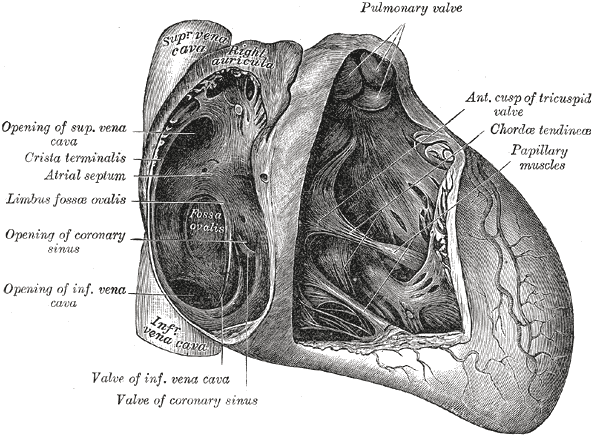
McKay T, Thomas L. Prominent crista terminalis and Eustachian ridge in the right atrium: Two dimensional (2D) and three dimensional (3D) imaging. European journal of echocardiography : the journal of the Working Group on Echocardiography of the European Society of Cardiology. 2007 Aug:8(4):288-91
[PubMed PMID: 16621718]
[6]
Sanjeev S, Karpawich PP. Superior vena cava and innominate vein dimensions in growing children : an aid for interventional devices and transvenous leads. Pediatric cardiology. 2006 Jul-Aug:27(4):414-9
[PubMed PMID: 16830087]
[7]
Nadesan T, Keough N, Suleman FE, Lockhat Z, van Schoor AN. Apprasial of the surface anatomy of the Thorax in an adolescent population. Clinical anatomy (New York, N.Y.). 2019 Sep:32(6):762-769. doi: 10.1002/ca.23351. Epub 2019 Mar 3
[PubMed PMID: 30758865]
[8]
Vuillemin M, Pexieder T. Normal stages of cardiac organogenesis in the mouse: II. Development of the internal relief of the heart. The American journal of anatomy. 1989 Feb:184(2):114-28
[PubMed PMID: 2712003]
[9]
Sondermeijer BM, Macgillavry MR, Tan HL. Left superior vena cava, a remnant of embryological development. Netherlands heart journal : monthly journal of the Netherlands Society of Cardiology and the Netherlands Heart Foundation. 2008 May:16(5):173-4
[PubMed PMID: 18566698]
[10]
Schauerte P, Mischke K, Plisiene J, Waldmann M, Zarse M, Stellbrink C, Schimpf T, Knackstedt C, Sinha A, Hanrath P. Catheter stimulation of cardiac parasympathetic nerves in humans: a novel approach to the cardiac autonomic nervous system. Circulation. 2001 Nov 13:104(20):2430-5
[PubMed PMID: 11705820]
[11]
Qin M, Zhang Y, Liu X, Jiang WF, Wu SH, Po S. Atrial Ganglionated Plexus Modification: A Novel Approach to Treat Symptomatic Sinus Bradycardia. JACC. Clinical electrophysiology. 2017 Sep:3(9):950-959. doi: 10.1016/j.jacep.2017.01.022. Epub 2017 Apr 26
[PubMed PMID: 29759719]
Level 2 (mid-level) evidence
[12]
Manousiouthakis E, Mendez M, Garner MC, Exertier P, Makita T. Venous endothelin guides sympathetic innervation of the developing mouse heart. Nature communications. 2014 May 29:5():3918. doi: 10.1038/ncomms4918. Epub 2014 May 29
[PubMed PMID: 24875861]
[13]
Phillippi JA. On vasa vasorum: A history of advances in understanding the vessels of vessels. Science advances. 2022 Apr 22:8(16):eabl6364. doi: 10.1126/sciadv.abl6364. Epub 2022 Apr 20
[PubMed PMID: 35442731]
Level 3 (low-level) evidence
[14]
Gustapane S, Leombroni M, Khalil A, Giacci F, Marrone L, Bascietto F, Rizzo G, Acharya G, Liberati M, D'Antonio F. Systematic review and meta-analysis of persistent left superior vena cava on prenatal ultrasound: associated anomalies, diagnostic accuracy and postnatal outcome. Ultrasound in obstetrics & gynecology : the official journal of the International Society of Ultrasound in Obstetrics and Gynecology. 2016 Dec:48(6):701-708. doi: 10.1002/uog.15914. Epub 2016 Nov 1
[PubMed PMID: 26970258]
Level 1 (high-level) evidence
[15]
Batouty NM, Sobh DM, Gadelhak B, Sobh HM, Mahmoud W, Tawfik AM. Left superior vena cava: cross-sectional imaging overview. La Radiologia medica. 2020 Mar:125(3):237-246. doi: 10.1007/s11547-019-01114-9. Epub 2019 Dec 10
[PubMed PMID: 31823296]
Level 2 (mid-level) evidence
[16]
Azizova A, Onder O, Arslan S, Ardali S, Hazirolan T. Persistent left superior vena cava: clinical importance and differential diagnoses. Insights into imaging. 2020 Oct 15:11(1):110. doi: 10.1186/s13244-020-00906-2. Epub 2020 Oct 15
[PubMed PMID: 33057803]
[17]
Demos TC, Posniak HV, Pierce KL, Olson MC, Muscato M. Venous anomalies of the thorax. AJR. American journal of roentgenology. 2004 May:182(5):1139-50
[PubMed PMID: 15100109]
[18]
Albay S, Cankal F, Kocabiyik N, Yalcin B, Ozan H. Double superior vena cava. Morphologie : bulletin de l'Association des anatomistes. 2006 Mar:90(288):39-42
[PubMed PMID: 16929820]
[19]
Farazi-Chongouki C, Dalianoudis I, Ninos A, Diamantopoulos P, Filippou D, Pierrakakis S, Skandalakis P. Double superior vena cava: presentation of two cases and review of the literature. Acta chirurgica Belgica. 2019 Oct:119(5):316-321. doi: 10.1080/00015458.2018.1438564. Epub 2018 Feb 19
[PubMed PMID: 29458311]
Level 3 (low-level) evidence
[20]
Raut MS, Das S, Sharma R, Daniel E, Motihar A, Verma A, Kar S, Maheshwari A, Shivnani G, Kumar A. Superior vena cava clamping during thoracic surgery: Implications for the anesthesiologist. Annals of cardiac anaesthesia. 2018 Jan-Mar:21(1):85-87. doi: 10.4103/aca.ACA_125_17. Epub
[PubMed PMID: 29336403]
[21]
De Raet JM, Vos JA, Morshuis WJ, van Boven WJ. Surgical management of superior vena cava syndrome after failed endovascular stenting. Interactive cardiovascular and thoracic surgery. 2012 Nov:15(5):915-7. doi: 10.1093/icvts/ivs316. Epub 2012 Jul 27
[PubMed PMID: 22843656]
[22]
Wilson LD, Detterbeck FC, Yahalom J. Clinical practice. Superior vena cava syndrome with malignant causes. The New England journal of medicine. 2007 May 3:356(18):1862-9
[PubMed PMID: 17476012]
[23]
Yu JB, Wilson LD, Detterbeck FC. Superior vena cava syndrome--a proposed classification system and algorithm for management. Journal of thoracic oncology : official publication of the International Association for the Study of Lung Cancer. 2008 Aug:3(8):811-4. doi: 10.1097/JTO.0b013e3181804791. Epub
[PubMed PMID: 18670297]
[24]
Katabathina VS, Restrepo CS, Betancourt Cuellar SL, Riascos RF, Menias CO. Imaging of oncologic emergencies: what every radiologist should know. Radiographics : a review publication of the Radiological Society of North America, Inc. 2013 Oct:33(6):1533-53. doi: 10.1148/rg.336135508. Epub
[PubMed PMID: 24108550]
[25]
Sheth S, Ebert MD, Fishman EK. Superior vena cava obstruction evaluation with MDCT. AJR. American journal of roentgenology. 2010 Apr:194(4):W336-46. doi: 10.2214/AJR.09.2894. Epub
[PubMed PMID: 20308479]
[26]
Keshvani N, Yek C, Johnson DH. Pemberton's sign in SVC syndrome from metastatic renal cell carcinoma. BMJ case reports. 2018 Mar 28:2018():. pii: bcr-2018-224190. doi: 10.1136/bcr-2018-224190. Epub 2018 Mar 28
[PubMed PMID: 29593001]
Level 3 (low-level) evidence
[27]
Kalra M, Gloviczki P, Andrews JC, Cherry KJ Jr, Bower TC, Panneton JM, Bjarnason H, Noel AA, Schleck C, Harmsen WS, Canton LG, Pairolero PC. Open surgical and endovascular treatment of superior vena cava syndrome caused by nonmalignant disease. Journal of vascular surgery. 2003 Aug:38(2):215-23
[PubMed PMID: 12891100]
[28]
Niazi AK, Reese AS, Minko P, O'Donoghue D, Ayad S. Superior Vena Cava Syndrome and Otorrhagia During Cardiac Surgery. Cureus. 2019 May 5:11(5):e4602. doi: 10.7759/cureus.4602. Epub 2019 May 5
[PubMed PMID: 31309025]
[29]
Nunnelee JD. Superior vena cava syndrome. Journal of vascular nursing : official publication of the Society for Peripheral Vascular Nursing. 2007 Mar:25(1):2-5; quiz 6
[PubMed PMID: 17324762]
[30]
Fagedet D, Thony F, Timsit JF, Rodiere M, Monnin-Bares V, Ferretti GR, Vesin A, Moro-Sibilot D. Endovascular treatment of malignant superior vena cava syndrome: results and predictive factors of clinical efficacy. Cardiovascular and interventional radiology. 2013 Feb:36(1):140-9. doi: 10.1007/s00270-011-0310-z. Epub 2011 Dec 7
[PubMed PMID: 22146975]



{kind=link}