Introduction
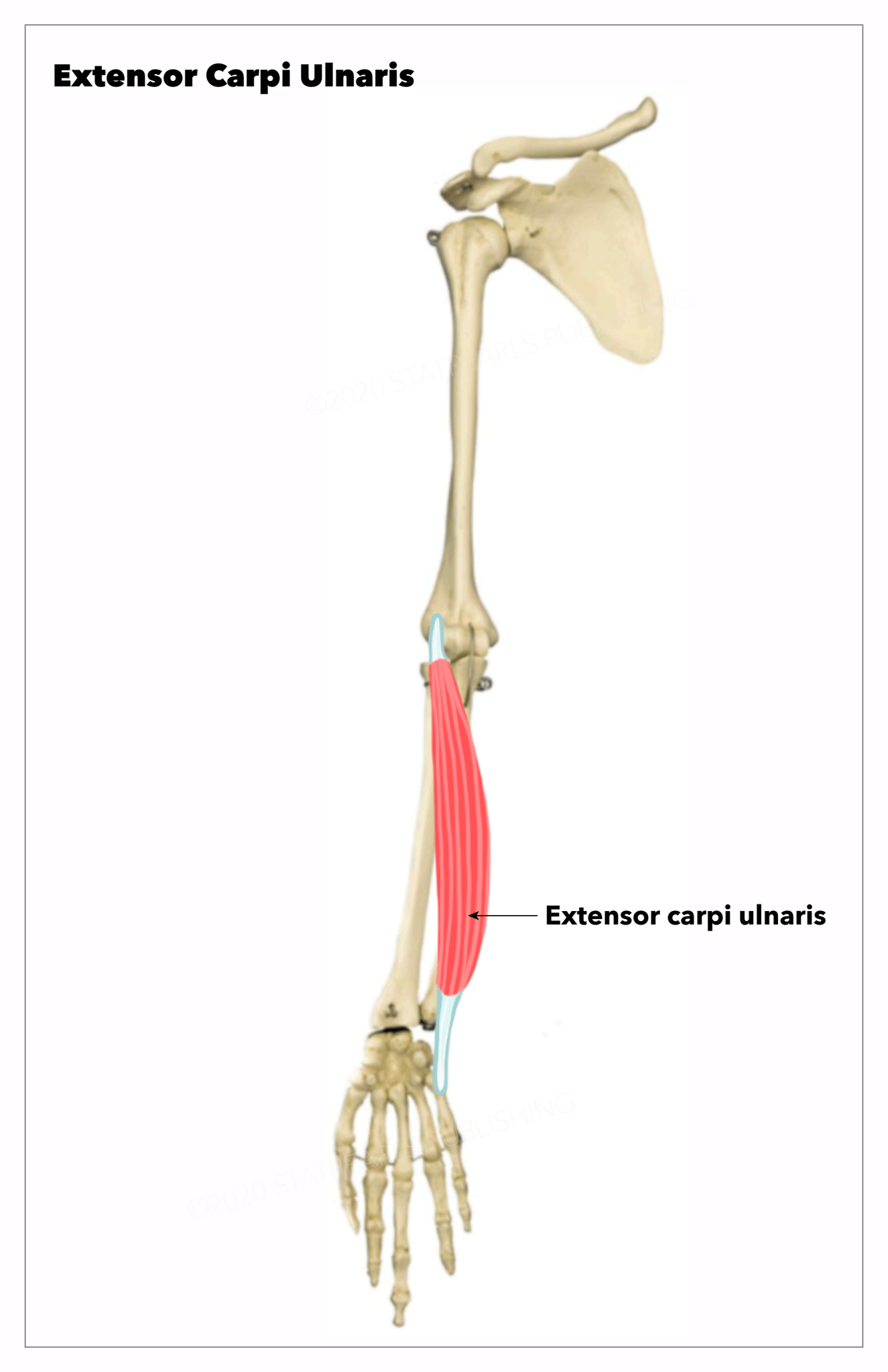
The extensor carpi ulnaris muscle is an elongated fusiform muscle located in the posterior compartment of the forearm and primarily functions to extend and adduct the wrist. It spans between the elbow and the base of the little finger. The extensor carpi ulnaris muscle belongs to the superficial group of extensors of the forearm along with brachioradialis, anconeus, extensor carpi radialis longus, extensor carpi radialis brevis, extensor digitorum, and extensor digiti minimi.
Its origin lies in the lateral epicondyle of the distal humerus and the posterior aspect of the ulna. It inserts onto the dorsal base of the fifth metacarpal after passing through the sixth compartment of the extensor retinaculum. It receives its innervation from the posterior interosseous nerve and gets its blood supply from the ulnar artery.[1]
Structure and Function
Structure
The extensor carpi ulnaris muscle has two heads, i.e., a humeral head and an ulnar head. The humeral head originates from the common extensor tendon and is attached to the lateral epicondyle of the humerus. The ulnar head derives from the common aponeurosis attached to the posterior border of the ulna. This common extensor tendon is shared by the flexor carpi ulnaris, flexor digitorum profundus, and deep fascia of the forearm. Distally, just proximal to the wrist, the extensor carpi ulnaris tendon, within the tendinous sheath of the extensor carpi ulnaris, runs beneath the extensor retinaculum in a groove between the posterior surface of the head and the styloid process of the ulna, which forms a separate compartment of the extensor retinaculum.
Relations
The extensor carpi ulnaris is the most medial muscle of the extensor compartment of the forearm; however, only a small triangular shape muscle called anconeus lies medially to the superior fibers of the extensor carpi ulnaris. Laterally, the extensor carpi ulnaris is related to the extensor digiti minimi and the extensor digitorum muscles. Distally, the cutaneous branch of the ulnar artery arises from between the tendons of the extensor carpi ulnaris and the flexor carpi ulnaris.
Functions
The extensor carpi ulnaris serves two functions. It extends the hand at the wrist joint by acting along extensor carpi radialis longus and extensor carpi radialis brevis. Along with the flexor carpi ulnaris, the extensor carpi ulnaris adducts the hand at the wrist. The simultaneous action of extensor carpi radialis longus and extensor carpi radialis brevis along with extensor carpi ulnaris helps to provide medial stability to the wrist while clenching the fist (tight flexion of the medial four digits).
Embryology
The forearm muscles originate in the dorsolateral somite cells that form muscles after they migrate to the limb at approximately the fourth week of development. As the limb buds lengthen, the muscles begin to divide into separate functional groups, such as the flexors and extensors. The anterior and posterior pattern of the limb develops by a sonic hedgehog protein, which gets secreted from the zone of polarizing activity.[2]
Blood Supply and Lymphatics
The extensor carpi ulnaris gets its vascular supply primarily from the ulnar artery, which branches off the brachial artery near the antecubital fossa and supplies the medial aspect of the forearm. Due to the muscle's location in the posterior compartment of the forearm, it also receives some blood supply from the posterior interosseous artery, a posterior branch of the radial artery that runs between the superficial and deep extensor muscle groups, supplying both.
The lymphatic drainage of the upper limb consists of both superficial and deep lymphatic vessels. The superficial lymphatic vessels of the hand and forearm ascend the arm along with the superficial veins, such as the basilic vein, and enter the cubital lymph nodes near the medial epicondyle of the humerus. Superficial lymphatic vessels traveling more proximally to the cephalic vein primarily drain into the apical axillary lymph nodes, though the deltopectoral lymph nodes are another potential drainage site. The deep lymphatic vessels of the arm and forearm follow the deep veins and end up in the humeral axillary lymph nodes and, eventually, the subclavian lymphatic trunk.[3]
Nerves
The muscle receives its nerve supply from the posterior interosseous nerve (C7-C8), a motor branch of the radial nerve. The radial nerve dives posteriorly through the heads of the supinator muscle in the antecubital fossa to form the posterior interosseous nerve. It innervates the extensor carpi ulnaris muscle in addition to the other muscles in the posterior compartment of the forearm. The radial nerve arises from the brachial plexus via the posterior cord, which has contributions from the spinal nerve roots of C5 to T1.[4]
Muscles
The extensor carpi ulnaris is one of the extensor muscles of the forearm located in the superficial layer of the posterior compartment of the forearm. It shares this compartment with the brachioradialis, the extensor carpi radialis longus, the extensor carpi radialis brevis, the extensor digitorum, and the extensor digiti minimi. These muscles all share a common origin on the lateral epicondyle via the common extensor tendon. As all of these muscles near their distal insertion sites, they are secured by the extensor retinaculum.
Physiologic Variants
Accessory tendinous slips of the extensor carpi ulnaris are present in some individuals, potentially predisposing them to injury. It can potentially prolong the symptoms of extensor carpi ulnaris syndrome, increase the risk of tendinopathy and dislocation of the muscle, and functionally limit the wrist and fifth digit.[5]
There are three variants of the accessory slip, types A, B, and C. Type A has been the most commonly identified and inserts into the base of the fifth metacarpal. Type B inserts onto the midshaft of the fifth metacarpal, and Type C inserts onto the fifth metacarpal head.[6] It is an accessory digiti minimi functionally that arises from the extensor carpi ulnaris.[7]
Surgical Considerations
The anatomic location of the extensor carpi ulnaris is essential in a variety of orthopedic procedures, including those operations at the level of the distal humerus, elbow joint, forearm, and wrist. For example, during the open reduction and internal fixation of the olecranon and proximal ulnar fractures, the extensor carpi ulnaris is identified based on its original fibers on the lateral epicondyle and dorsal aspect of the ulna and may need to be manipulated to locate the components of the fracture.
One of the injuries that may require surgical intervention is the subluxation of the extensor carpi ulnaris. It more frequently occurs in athletes subject to frequent, forceful wrist rotation than in the general population. This injury most commonly occurs in sports such as tennis, golf, and water polo.[8] The dislocation occurs with the supination of the forearm due to a torn fibro-osseous sub sheath that encompasses the tendon. This sheath is a part of the sixth compartment of the extensor retinaculum that anchors to the distal ulna.
Three different types of retinacular tears can contribute to this condition described in the literature. Type A involves the ulnar rupture of the sheath in which the sheath remains superficial to the tendon. Type B describes a radial rupture of the sheath in which it lies in the ulnar groove of the bone. Lastly, type C occurs when the fibro-osseous sheath is detached from the periosteum of the ulna, thus forming a false pouch for the tendon.[9]
Patients with this injury often describe a painful snap at the dorsal-ulnar aspect of the wrist. There is some controversy concerning the treatment of this injury. However, surgical repair of the fibro-osseous sheath is effective.[10] For the radial rupture of the fibro-osseous sheath securing the tendon, the patients can be effectively treated via direct suturing of the sheath over the tendon. For the ulnar rupture of the sheath, patients undergo a reconstruction of the sheath with the existing extensor retinaculum. Upon successfully completing this surgery, patients can return to their previous level of functioning in their respective sports without pain or recurrent dislocation.[11]
Clinical Significance
The extensor carpi ulnaris is an essential muscle in the activity of the wrist and forearm that contributes not only to the extension and adduction of the wrist but also to its medial stability. It is most commonly injured in athletes subject to forceful wrist movements. Repetitive flexion and extension of the wrist can lead to tenosynovitis due to the irritation of the tendon and the sheath that holds it in place. Overuse can also lead to tendinopathy of the muscle's tendon, in which there can be thickening and painful stiffness of the tendon with minimal structural damage. Continued excessive stress on the tendon can cause structural damage, which can lead to a partial tear.[1]
Testing the Function of Extensor Carpi Ulnaris Muscle
For testing the extensor carpi ulnaris muscle's function or instability, ask the patient to pronate the forearm and extend the fingers. Place your hand along the medial border of the hand to provide resistance against the movement. The extended wrist is then adducted against resistance. The muscle can be seen and felt in the proximal part of the forearm, and its tendon can be palpated proximal to the head of the ulna if the muscle is acting normally.[12]
Other Issues
Acute tendon ruptures are uncommon and are typically the result of a penetrating injury.[1]