Continuing Education Activity
Buckle fractures are incredibly common injuries that present to the emergency department, which are invariably always managed conservatively, and do not routinely require orthopedic input. This activity outlines the evaluation and management of pediatric buckle fractures and reviews the role of the healthcare team in managing patients with this condition.
Objectives:
- Summarize the management considerations for patients with buckle fractures.
- Describe imaging findings associated with buckle fractures.
- Identify reasons for delayed diagnosis of buckle fractures.
- Explain how to counsel a patient with a buckle fracture.
Introduction
The pediatric skeletal anatomy has unique properties that lead to varied pathology to that of the adult skeleton. Two of the major differences include the presence of the physeal growth plate and a thicker periosteum with the softer underlying bone.[1] With soft, malleable bone, and a thick protective periosteal covering, minor injuries can result in a spectrum of deformities with or without a cortical break. In long bones, injuries without a cortical break either lead to plastic deformation through microfracture or to a ‘kink’ within the long bone, described as a ‘buckle’ or ‘torus’ fracture.
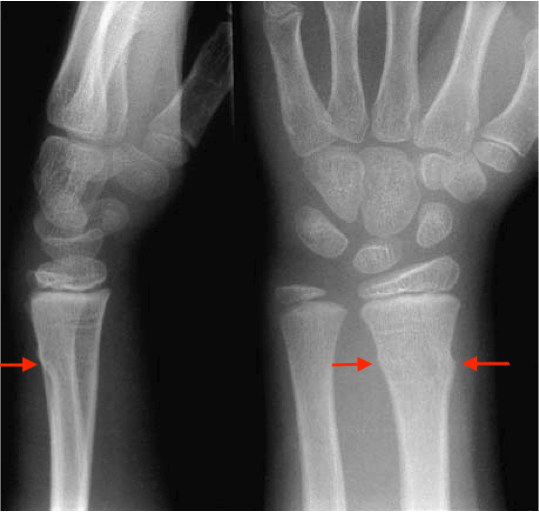
The appearance on plain X-ray shows the fracture site as two outcroppings of bone, as though the long bone has collapsed or ‘buckled.’ The word "torus" is the Latin word "protuberance. However, if there is a fracture with a cortical breach, it is termed a greenstick fracture if unicortical or a complete fracture if bicortical.
Buckle fractures are incredibly common injuries that present to the emergency department, which are invariably always managed conservatively, and do not routinely require orthopedic input.
Etiology
Buckle fractures occur almost exclusively in long bones of children, although they can also occur in flat bones - particularly rib fractures.[2] The distal radius is among the most commonly broken bones during childhood. The mechanism of injury is by axial loading, which frequently occurs due to falling on an outstretched arm.
Epidemiology
Of all pediatric injuries, fractures constitute around 25% of hospital attendance.[3] Distal radius and buckle fractures make up 27.2%, which, by far, is the most common bone to be injured and sustain a buckle fracture.[4] Specifically, 50% of pediatric wrist fractures are buckle fractures.[5] These injuries occur throughout the pediatric age range but are particularly common between the ages of 7 to 12 years old.[4]
History and Physical
The history and physical examination of these injuries are relatively simple. As with any trauma history, the mechanism of injury is of utmost importance. Like with every trauma case, one should ascertain if there are any other injuries and to make sure this is not a distracting injury to something more pressing.
During the physical examination, inspection is key, and one must assess for any clinical deformities. Additionally, general principles for the assessment of any bruising, swelling, or bony tenderness around the site of injury may indicate a fracture. One must also be aware that although radiographs may show a buckle fracture if a clinical deformity exists, there may also be a plastic deformation that requires correction.
Finally, with children, one must always be wary of non-accidental injury (NAI). Therefore, an ever-present high index of suspicion is required, particularly if any inconsistencies in the history, delayed presentation, multiple injuries of different ages, or if the mechanism of injury does not equate to the given fracture pattern.
Evaluation
Two plain radiographs in two orthogonal planes are required to assess the fracture site for any cortical breach and level of deformity. Typical X-ray findings would include buckling out of one or both cortexes in a long bone, with or without deformity. Also, there may be a plastic deformation of an associated bone – e.g., the ulna in distal radius fractures. If there is a suspicion of plastic deformation, one might obtain an X-ray of the contralateral limb for comparison.
Additionally, depending on the mechanism of injury and symptoms, one may also require radiographs more proximally to assess for any associated injury. For example, an associated injury to a distal radius buckle fracture could be supracondylar fractures or radial head fractures/dislocations. Thus, as a rule of thumb, always assess for injuries in joints above and below the fracture site.
Treatment / Management
Treatment goals in buckle fractures are for patient comfort and parental reassurance. These are inherently stable injuries and almost never require any further intervention.[6][7]
Following an adequate history and physical examination, if the relevant X-rays show an isolated injury, then the treatment is with removable wrist splints, a pre-fabricated removable cast, or a soft cast that can be removed once at home by the parents once the treatment has finished. This splinting/casting is usually only necessary for two to three weeks because these fractures are considered stable.
Evidence from RCTs have shown removable splints to be the best treatment, which offers easier use for daily activities, better physical function, and are generally preferred by patient and parent in comparison to below elbow casting.[8][9] Thus, these patients can be safely discharged with appropriate parental counseling on the removal of the splint/soft cast and to avoid any contact sports or dangerous activities for six to eight weeks from injury.[10]
Ideally, the treatment mentioned above is offered in the emergency department, and the patient is discharged, but in many cases, they are often referred onwards to fracture clinics for follow-up.
Differential Diagnosis
- Buckle fracture
- Greenstick fracture
- Salter-Harris fracture
- Toddler’s fractures – undisplaced spiral fractures of the distal tibia
- Plastic deformation
- Soft tissue injury
- Non-accidental injury
Prognosis
Of all pediatric fractures, buckle fractures have an excellent prognosis. They are inherently stable, without any real risk of displacement or long-term sequelae, largely due to an intact, thick periosteum around the entire cortex. Also, there is excellent remodeling potential at the distal radius.[11] Therefore, these patients can be safely discharged after their first presentation without the need for follow-up.
Complications
Complications are rare and do not relate to the actual injury but rather to the treatment. Some authors have noted rare incidences of blistering or joint stiffness due to prolonged use of non-removable casts. Thus, the preference for treatment has shifted towards removable wrist splints or pre-fabricated removable casts.
Deterrence and Patient Education
These injuries are almost inevitable due to the nature of children’s play and the increased incidence of falling on outstretched hands. However, in such cases, prompt evaluation of the site of injury is warranted to rule out fractures and treatment with removable casts. A key component would include parental education on the correct method of management of the soft casts. High-risk activities such as contact sports, or anything with a high risk of falling, should be avoided after injury for a period of up two months to prevent further injury.
Enhancing Healthcare Team Outcomes
Buckle fractures present uniquely in the pediatric population, and a multidisciplinary approach is necessary. This approach would include triage and initial treatment through the emergency department, casting or application of a wrist splint by plaster technicians, and though not necessarily required, almost invariably review in the fracture clinic by an orthopedic surgeon.
The key to efficiency in their management is recognition of this injury in the emergency department and treatment into a splint/soft cast and discharge to avoid unnecessary hospital visits. The parents must receive adequate counseling on the child's condition and recovery.