Introduction
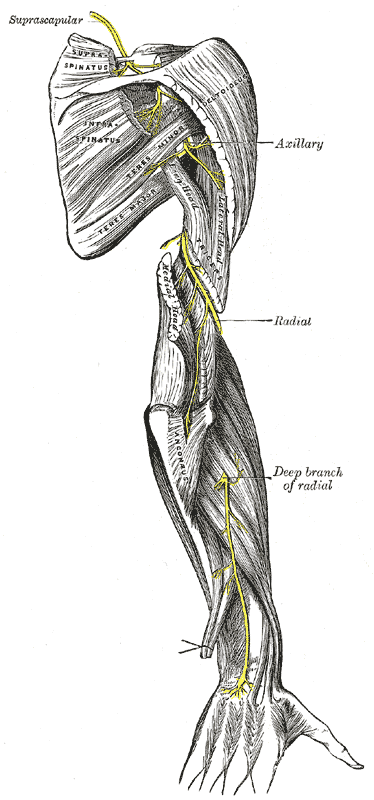
The radial nerve is a peripheral nerve supplying specific parts of the arm, forearm, wrist, and hand (see Image. Posterior Upper Extremity Nerves). This nerve has both motor and sensory functions. The motor branches stimulate the posterior arm muscles, posterior forearm muscles, and extrinsic wrist and hand extensors. The sensory branches supply the skin on the anterolateral arm, distal posterior arm, posterior forearm, and posterolateral wrist and hand areas. The radial nerve's distribution diminishes lateromedially from the thumb to the ring finger. The median nerve innervates the digit pads of the lateral 3-1/2 fingers, while the ulnar nerve supplies the medial 1-1/2 digit pads.
The radial nerve originates from the ventral rami of the spinal nerves C5 to T1 and is part of the posterior cord of the brachial plexus. Radial nerve disruption can lead to neurologic deficits in its area of distribution.[1]
Structure and Function
Radial Nerve Structure
The radial nerve is the continuation of the brachial plexus' posterior cord and has contributions from the C5 to T1 nerve fibers. It exits the axilla and then sequentially courses through the posterior arm, anterior arm, and posterior forearm compartments.[2]
Radial nerve in the arm
The radial nerve exits the axilla posterior to the brachial artery and then enters the posterior arm compartment through the triangular interval. The triangular interval is bounded by the triceps brachii's long head medially, the teres major superiorly, and the humerus laterally.
In the arm, this posterior cord derivative runs between the triceps' long and medial heads before giving branches to the long and lateral heads of the muscle. Further distally, it passes around the humerus' radial groove together with the profunda brachii (deep brachial) artery. At this level, the radial nerve sends a branch to the medial head of the triceps.
At the lateral aspect of the humerus, the nerve pierces the lateral intermuscular septum and then travels anteroinferiorly between the brachialis and brachioradialis at the cubital fossa. Anterior to the lateral humeral epicondyle, the radial nerve bifurcates into a deep motor-articular branch and a superficial cutaneous-articular branch.[3]
Radial nerve in the forearm
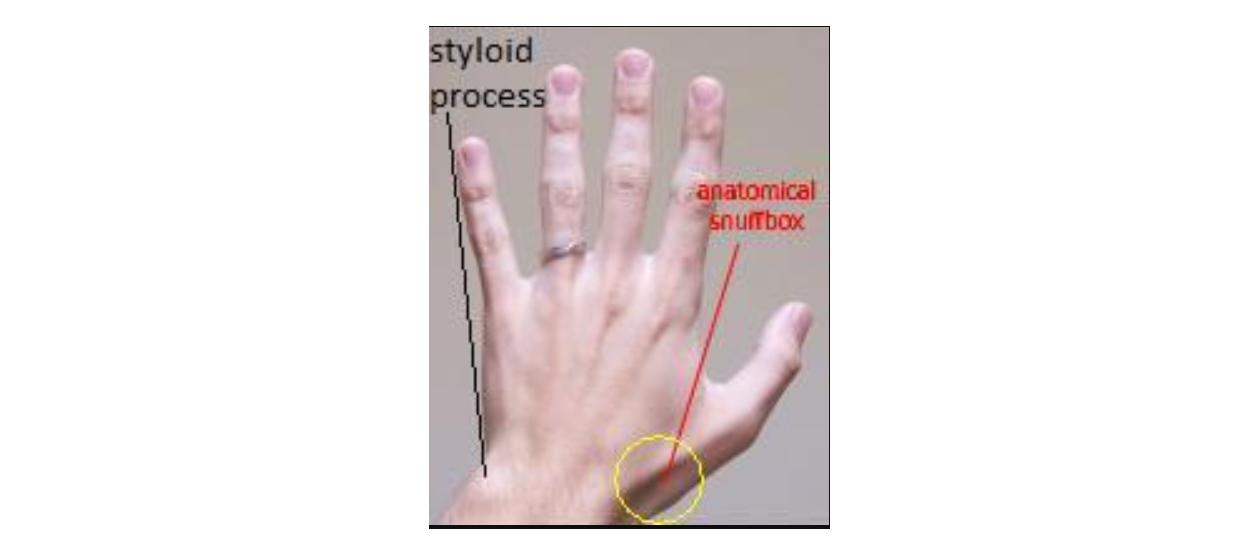
In the forearm, the radial nerve's superficial branch descends deep to the brachioradialis. It then crosses the anatomic snuff box distally (see Image. Anatomical Snuff Box and Ulnar Styloid Process). This nerve supplies the skin and joints of the dorsal aspect of the hand and lateral 3-1/2 digits.
Meanwhile, the deep branch of the radial nerve pierces the supinator, travels around the lateral margin of the radius' neck, and enters the posterior forearm compartment. This branch is the distal continuation of the radial nerve and supplies the posterior forearm muscles. Further distally, the deep branch of the radial nerve becomes the posterior interosseous nerve, which passes deep to the extensor pollicis longus and terminates on the interosseous membrane.
The radial nerve gives off a third branch in the forearm, the posterior cutaneous nerve of the forearm. This nerve supplies the skin on the posterior aspect of the forearm and wrist.[3]
Radial nerve in the hand
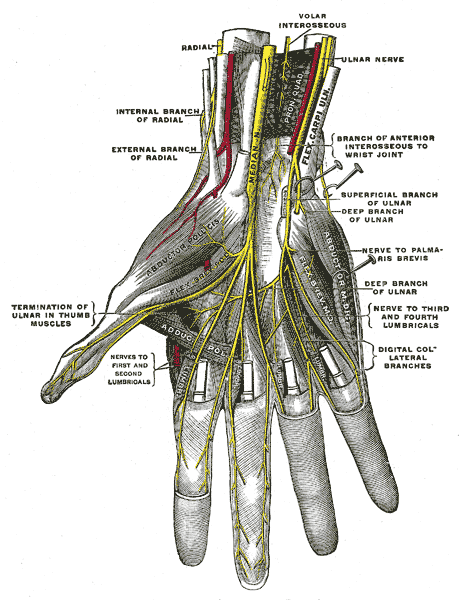
The only branches of the radial nerve in the hand come from its superficial sensory branch, which originates from the cubital fossa. Hand extensors are extrinsic muscles originating from the forearm and innervated by the deep branch of the radial nerve (see Image. Nerves In The Hand).
Radial Nerve Functions
The following is a list of the motor and cutaneous sensory functions of the radial nerve.
Sensory distribution
- Anterior aspect
- Inferior lateral cutaneous nerve of the arm: anterior lateral aspect of the mid-arm
- Posterior aspect
- Posterior cutaneous nerve of the arm: posterior distal arm
- Posterior cutaneous nerve of the forearm: a strip on the posterior aspect of the forearm
- Superficial branch: posterior aspect of the lateral 3-1/2 digits and dorsal hand area
Motor distribution
- Radial nerve
- Triceps brachii (medial, lateral, and long heads): forearm extension
- Extensor carpi radialis longus: wrist extension
- Brachioradialis: elbow flexion and forearm pronation and supination, depending on the forearm's position
- Anconeus: elbow extension
- Deep branch of the radial nerve
- Extensor carpi radialis brevis: wrist extension and abduction
- Supinator: forearm supination
- Posterior interosseous nerve
- Abductor pollicis longus: thumb abduction at the wrist
- Extensor carpi ulnaris: wrist extension and adduction
- Extensor digiti minimi: 5th digit and wrist extension
- Extensor digitorum: extension of the medial 4 hand digits
- Extensor indicis: index finger and wrist extension
- Extensor pollicis brevis: thumb extension and abduction at the carpometacarpal and metacarpophalangeal joints
- Extensor pollicis longus: extension of the thumb's terminal phalanx
Embryology
The radial nerve arises from the bilaterally paired neural crest—the strips of ectodermal cells at the neural tube margins in the embryo. Neural crest cell migration to the upper limb gives rise to the peripheral nerves, including the radial nerve.[4]
Blood Supply and Lymphatics
The radial nerve exits the axilla together with the brachial artery, which is the axillary artery's continuation at the lower border of the teres major. Further distally, the nerve enters the posterior arm compartment through the triangular interval together with the deep brachial artery. The radial nerve follows the radial collateral artery until it passes anteriorly over the cubital fossa. The nerve gives off a superficial branch at the cubital fossa, which runs alongside the radial artery, deep branch of the radial artery, and posterior interosseous artery.[5]
Nerves
The radial nerve is the direct continuation of the posterior cord and the biggest terminal branch of the brachial plexus. This nerve is derived from C5 to T1 nerve roots and has the following branches:[6]
Sensory
- Inferior lateral cutaneous nerve of the arm
- Posterior cutaneous nerve of the arm
- Posterior cutaneous nerve of the forearm
- Superficial branch of the radial nerve
Motor
- Deep branch of the radial nerve
- Posterior interosseous nerve
Muscles
The radial nerve and its branches innervate the following muscles:[7]
- Abductor pollicis longus
- Anconeus
- Brachioradialis
- Extensor carpi radialis brevis
- Extensor carpi radialis longus
- Extensor carpi ulnaris
- Extensor digiti minimi
- Extensor digitorum
- Extensor pollicis brevis
- Extensor indicis
- Extensor pollicis longus
- Triceps brachii (medial, long, and lateral heads)
- Supinator
The specific nerve branch distributions and muscle actions are explained above in the Structure and Function section.
Physiologic Variants
The deep branch of the radial nerve normally passes between the supinator's heads, where it becomes the posterior interosseous nerve and innervates the posterior forearm muscles. However, in some individuals, the deep branch of the radial nerve passes through the arcade of Frohse (supinator arch), which can increase the likelihood of impingement.[8][9][10]
Surgical Considerations
Iatrogenic radial nerve damage can produce neurologic deficits distal to the injury site. Radial nerve tears at the level of the brachial plexus may result from sternal retraction, ie, during internal mammary artery dissection and cardiac surgery. Elbow hyperextension, eg, during upper extremity surgery or when in a supine position for long intervals, risks radial nerve damage at this level. Preventing elbow-level radial injury in an anesthetized patient requires slight elbow flexion. Damage to the superficial radial nerve is a potential complication of treating de Quervain tendinopathy surgically.[3][11]
Clinical Significance
Various conditions may affect the radial nerve and produce neurologic deficits in its areas of distribution. This section discusses unique and common cases encountered in practice.
Radial Nerve Palsy
Radial neuropathies commonly arise from radial nerve injury due to compression, ischemia, arm fractures, penetrating wounds, and surgical complications. Symptom severity depends on the level of the injury. Wrist drop, or the inability to extend the hand, is the most common presentation. Other names for radial nerve palsy include "crutch palsy," "Saturday night palsy," and "honeymooner’s palsy," all of which suggest prolonged compression of the radial nerve near or at the axillary level.[12][13][14]
Radial Nerve Entrapment
The radial nerve can get injured or compressed anywhere along its path. Consequently, pain followed by sensory and motor deficits may manifest in the areas this nerve supplies. The proximal forearm is a commonly compressed site where the posterior interosseous branch of the radial nerve passes between the supinator heads.
Less commonly involved sites are the middle and proximal thirds of the humeral shaft, as occurs during humeral fractures, and the radial aspect of the wrist. The treatment depends on the pathology. Conservative management is given for mild injuries, while surgery is reserved for severe or refractory cases.[12][13]
Cheiralgia Paresthetica (Wartenberg Syndrome)
Cheiralgia paresthetica is a hand neuropathy commonly caused by trauma or compression of the superficial branch of the radial nerve. The dorsum of the hand near the anatomical snuffbox is typically affected, though it may also involve the dorsal aspect of the rest of the hand. Symptoms include pain, numbness, tingling, or a burning sensation. There is no motor involvement since the superficial branch is purely sensory. The etiology is thought to be wrist compression, such as with a watch band or bracelet. Association with handcuff use gives this condition the name "handcuff neuropathy."[15]
Radial Tunnel Syndrome
The radial tunnel is an area 5 cm in length, beginning at the radiocapitellar joint (lateral elbow) and terminating at the proximal border of the supinator. This area is close to the origin of the branches of the radial nerve in the forearm. Radial tunnel syndrome is an uncommon compression neuropathy affecting the radial nerve at this level. The condition typically arises from repetitive forearm movements, particularly supination and pronation, and is associated with certain occupations or sports activities.
Symptoms include fatigue or a dull, aching pain at the proximal portion of the forearm during use. Less commonly, pain may be felt at the dorsal aspect of the wrist or hand. Extensor and supinator weakness are usually not observed, as the radial nerve's cutaneous branches are most commonly affected.[16][17]
Posterior interosseus nerve compression syndrome is similar to radial tunnel syndrome. This neuropathy affects the posterior interosseus nerve, which innervates the supinator and wrist and hand extensors. Thus, it more commonly presents with motor deficits.[16][18]
Radial tunnel syndrome can be managed medically or surgically. The main surgical landmark for correcting radial tunnel syndrome is the radial head, specifically its palpable proximal aspect. The posterior interosseus nerve exits the superficial head of the supinator muscle 7.4 cm distal to this landmark.[8][13]
Posterior Interosseus Nerve Compression Syndrome
Posterior interosseus nerve compression syndrome differs from radial tunnel syndrome because it involves motor losses to the muscles innervated by the posterior interosseus nerve. Nerve compression occurs at the arcade of Frohse. Trauma, inflammation, and tumors are common causes of this neuropathy.[19][22]
Other Issues
The radial nerve lies in the radial groove of the humerus, making it vulnerable to injury after a humeral shaft fracture. Radial nerve damage at this level can cause wrist drop, a condition notable for the inability to extend the wrist. A lateral supracondylar fracture may also damage the radial nerve but will present differently from a midhumeral injury. Nerve branches to the brachioradialis and extensor carpi radialis longus arise above this fracture so that these muscles are largely unaffected. Instead of presenting with a wrist drop, the patient's wrist weakly extends radially when asked to extend the hand.[16][20][21]