Continuing Education Activity
Osteomalacia, often referred to as "soft bone disease," is a metabolic bone disorder characterized by the inadequate mineralization of bone tissue. This condition results from a deficiency in vitamin D, calcium, or phosphate, weakening and softening bones. Given that vitamin D deficiency is the most common nutritional deficiency among children and adults, this disorder is particularly relevant. While osteoporosis is a more widely recognized bone disorder, osteomalacia represents a distinct but equally significant concern within the realm of bone health. Understanding osteomalacia is crucial, as it can cause a range of debilitating symptoms and complications, including bone pain, muscle weakness, and an increased risk of fractures. This activity reviews the various facets of osteomalacia, from its causes and symptoms to diagnosis and treatment, shedding light on a condition that warrants attention within the broader landscape of skeletal health. This activity also highlights the role of an interprofessional team in optimizing care for patients affected by this condition.
Objectives:
Identify the various risk factors for developing osteomalacia.
Implement appropriate diagnostic tests, such as serum vitamin D levels, bone mineral density scans, and parathyroid hormone measurements, to confirm osteomalacia.
Apply evidence-based guidelines to select the most suitable treatment modalities, including vitamin D supplementation, dietary adjustments, and underlying disease management.
Collaborate with an interprofessional team to coordinate and enhance the delivery of care for patients with osteomalacia.
Introduction
Vitamin D deficiency is the most common nutritional deficiency among children and adults. Osteomalacia describes a disorder of “bone softening” in adults that is usually due to prolonged deficiency of vitamin D. This deficiency results in abnormal osteoid mineralization. In contrast, rickets results from deficient mineralization at the cartilage of growth plates in children.
Several cell types constitute bone and participate in the coordinated process of bone remodeling. Osteoclasts, bone-resorbing cells, break down bone by secreting collagenase. Osteoblasts deposit the osteoid matrix, a collagen scaffold in which inorganic salts are deposited to form mineralized bone. This intricate process is directly and indirectly influenced by hormonal signals, namely parathyroid hormone (PTH) and calcitonin, which act in response to serum calcium levels.
In processes that decrease the amount of vitamin D or its bioproducts, normal serum calcium will be maintained by mobilizing calcium from the bones. Specifically, PTH will be secreted by the parathyroid glands in response to hypocalcemia from vitamin D deficiency and will attempt to bring the body back to normal serum calcium levels. Bones are the primary target to recruit calcium, and osteomalacia will ensue by extracting calcium from the bones. Therefore, adults affected by processes that disrupt vitamin D metabolism and its production are at risk for eventually developing osteomalacia and its clinical manifestations.[1][2][3]
Etiology
Osteomalacia is a metabolic bone disease characterized by impaired mineralization of bone matrix. Bone creation occurs by the deposition of hydroxyapatite crystals on the osteoid matrix. Details of this disease's most common and sometimes overlooked causes are described below.
Decreased Vitamin D Production
- Cold weather climates reduce skin sunlight exposure and cutaneous synthesis.
- Dark skin and relatively increased melanin compete with 7-dehydrocholesterol ultraviolet-B (UVB) light absorption.
- Obesity can lead to increased adipose sequestration, which results in less calcidiol substrate available for activation.
- In older individuals, vitamin D production decreases, and in general, the storage of vitamin D declines with age.
Decreased Vitamin D Absorption
- Nutritional deficiency can cause vitamin D deficiency even with adequate sunlight exposure.
- Malabsorptive syndromes such as Crohn disease, cystic fibrosis, celiac disease, cholestasis, and surgical alteration of the gastrointestinal tract (ie, gastric bypass) are associated with deficient absorption of fat-soluble vitamins (A, D, E, and K).
Altered Vitamin D Metabolism
- Chronic kidney disease leads to structural damage, loss of 1-alpha-hydroxylase, and suppressed enzymatic activity secondary to hyperphosphatemia.
- Nephrotic syndrome leads to pathologic excretion of vitamin D binding protein (DBP), which binds to serum calcidiol.
- Liver disease (ie, cirrhosis, nonalcoholic fatty liver disease, nonalcoholic steatohepatitis) leads to deficient production of calcidiol.
- Pregnancy is associated with decreased calcidiol levels, and the American College of Obstetricians and Gynecologists recommends 1000 to 2000 international units (IU) per day for treating identified vitamin D deficiency in pregnant women.
Hypophosphatemia or Hypocalcemia
- Renal tubular acidosis, such as in Fanconi syndrome, alters ion absorption and excretion.
- Multiple IV iron infusions have been found to cause hypophosphatemia and osteomalacia.[4]
- Tumor-induced osteomalacia, also known as oncogenic osteomalacia, is a rare acquired paraneoplastic disease characterized by hypophosphatemia and renal phosphate wasting.[5][6][7]
- It is commonly caused by benign tumors involving the skin, muscles, bones of the extremities, or the paranasal sinuses.
Medications
- Antiepileptic drugs, including phenobarbital, phenytoin, and carbamazepine, enhance catabolism of calcidiol via induction of P-450 activity.[8]
- Isoniazid, rifampicin, and theophylline also precipitate vitamin D deficiency in the same manner as antiepileptic medications.
- Antifungal agents such as ketoconazole increase vitamin D requirements by inhibiting 1-alpha-hydroxylase (CYP27B1).
- Long-term steroid use also has implications for vitamin D deficiency, possibly by increasing 24-hydroxylase activity.[9][10][11][12]
Epidemiology
There are reports that the prevalence of osteomalacia histologically at post-mortem is as high as 25% in adult Europeans. However, the true incidence of osteomalacia remains largely underestimated across the globe. At-risk individuals include those with dark skin, limited sun exposure, low socioeconomic status, poor diet, and frequent wearers of full-body clothing. These risks vary worldwide and are contingent on geographic location, cultural preferences, and ethnicity. Healthcare professionals should take these factors, as well as other relevant clinical findings, into account when choosing to obtain further studies or recommending vitamin D supplementation.[13]
Pathophysiology
It is essential to review vitamin D metabolism to understand the pathologic processes that result in vitamin D deficiency and its subsequent manifestations (see Image. Vitamin D Metabolism).
The synthesis of active vitamin D (calcitriol) organically begins in the skin, where cholecalciferol (vitamin D3) is formed by the action of UVB radiation in epidermal keratinocytes and dermal fibroblasts converting 7-dehydrocholesterol (provitamin D3) to pre-vitamin D, which spontaneously isomerizes to form cholecalciferol.
Subsequently, cholecalciferol gets transported to the liver, where it is converted to calcidiol, 25-hydroxyvitamin D [25(OH)D], by 25-hydroxylase (CYP2R1). Therefore, it is logical that patients with chronic liver disease would be at risk of developing vitamin D deficiency. This particular form of vitamin D is partially water-soluble and has a short half-life. It is worth noting that 25(OH)D is also the best indicator of overall vitamin D status because this measurement accurately reflects total vitamin D levels from dietary intake, natural sunlight exposure, and converted adipose stores in the liver. Estimates are that approximately 40% to 50% of circulating 25(OH)D derives from skin conversion.
Enzymatic conversion to calcitriol, 1,25-dihydroxy-vitamin D [1,25(OH)D], occurs in the kidneys by 1-alpha-hydroxylase. Similarly, chronic renal disease, amongst other renal pathologies, can cause vitamin D deficiency, which is why secondary and, eventually, tertiary hyperparathyroidism can develop with long-term renal failure. It is important to realize that 1-alpha-hydroxylase activity is strictly regulated.
As with any synthetic biologic process, feedback loops exist to regulate calcitriol production, namely:
- Positive feedback by parathyroid hormone (PTH)
- Positive feedback by decreased serum phosphate levels
- Negative feedback by fibroblast growth factor 23 (FGF-23) is secreted by osteocytes in the bone matrix, inhibiting renal phosphate absorption.
- Negative feedback by calcitriol inhibition of 1-alpha-hydroxylase, which in turn decreases calcitriol synthesis and also stimulates 24-hydroxylase (CYP24R1) activity.
- 24-hydroxylase effectively removes circulating calcitriol by converting it to biologically inactive 24,25-dihydroxy vitamin D [24,25(OH)D].[14]
History and Physical
When evaluating for osteomalacia, a history should include a review of the patient's family history and surgical history. Other pertinent questions should focus on activity level, hobbies, diet (ie, vegetarian), and assessment of socioeconomic status.
Symptoms of osteomalacia are non-specific and may include the following:
- Proximal muscle weakness and wasting
- Myalgias and arthralgias
- Muscle spasms
- Altered or "waddling" gait
- Spinal, limb, or pelvic deformities (long-term osteomalacia)
- Aching bone pain (lower spine, pelvis, or lower extremities)
- Aggravated by activity and weight-bearing
- Increased falls
- Hypocalcemic seizures or tetany [15]
Evaluation
No single laboratory finding is specific for osteomalacia. However, patients with osteomalacia will usually have hypophosphatemia or hypocalcemia. Additionally, increased alkaline phosphatase activity is typically characteristic of diseases with impaired osteoid mineralization. Some sources believe that either hypophosphatemia or hypocalcemia and increased bone alkaline phosphatase levels are necessary to even suspect osteomalacia. Low bone mineral density (BMD) and focal uptake at Looser zones can appear on bone scintigraphy as the disease progresses. Below, the findings of definite or possible osteomalacia are described, as proposed by Fukumoto et al., which require validation with further studies.[16][17]
- Hypophosphatemia or hypocalcemia
- High bone alkaline phosphatase
- Muscle weakness or bone pain
- Less than 80% BMD of the young-adult-mean
- Multiple uptake zones by bone scintigraphy or radiographic evidence of Looser zones (pseudofractures)
*Definite osteomalacia is defined as having all of the above findings, numbers 1–5.
*Possible osteomalacia is defined as having the findings of numbers 1, 2, and 2 of the 3 numbers 3–5 findings described above.
In another review by Uday and Hogler, new criteria were proposed for the diagnosis of osteomalacia, and are as follows:
- Elevated PTH levels
- Elevated alkaline phosphatase levels
- Low urine calcium levels
- Low calcium intake (usually <300 mg/day) or low calcidiol levels (<30 nmol/L) [18]
The use of the above criteria can help with the diagnosis of osteomalacia only in cases where kidney or liver problems are lacking.
The serum level of 25(OH)D is currently regarded as the best marker of vitamin D status and is usually severely low (<10 ng/mL) in patients with nutritional osteomalacia. Other sensitive biomarkers of early calcium deprivation include increased serum PTH and decreased urinary calcium.
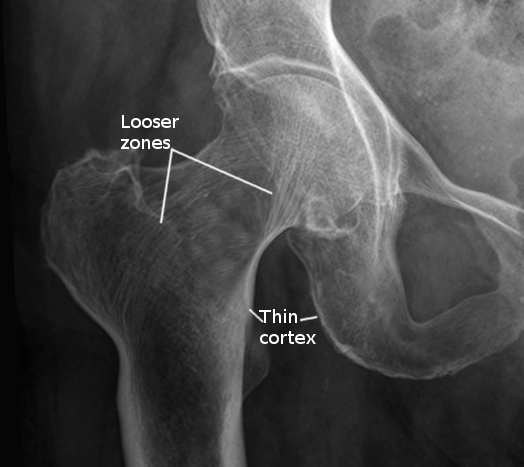
Radiographic findings may include Looser zones or pseudofractures, a classic finding in osteomalacia. They may represent poorly repaired insufficiency fractures and are visible as transverse lucencies perpendicular to the osseous cortex. They typically occur bilaterally and symmetrically at the femoral necks, shafts, pubic and ischial rami. Additionally, radiographs can show decreased distinctness of vertebral body trabeculae due to the inadequate mineralization of osteoid. Although not required for diagnosis, studies have demonstrated reduced bone mineral density in the spine, hip, and forearm (see Image. Osteomalacia Hip Joint ).
Iliac crest bone biopsy is considered the gold standard for establishing the diagnosis of osteomalacia. Still, it should be reserved for when the diagnosis is in doubt, or the cause of osteomalacia is equivocal by noninvasive methods.[16][19]
Treatment / Management
After establishing the diagnosis of osteomalacia, it is crucial to evaluate the etiology. Treatment should focus on reversing the underlying disorder and correcting the vitamin D and other nutritional or electrolyte deficiencies.
When the clinician has determined that vitamin D deficiency is the underlying cause of certain symptomatology, the treatment may significantly improve strength and relieve bone tenderness within weeks. Serum calcium and urine calcium levels should be monitored, initially after 1 and 3 months, and then every 6 to 12 months until 24-hour urine calcium excretion is normal. Serum 25(OH)D level can be measured 3 to 4 months after starting therapy. If hypercalcemia or hypercalciuria is present, the dose can be adjusted to prevent excessive vitamin D dosing.
For patients with severe vitamin D deficiency, below is a possible dosing approach:
- 50,000 IU of ergocalciferol (vitamin D2) or cholecalciferol (vitamin D3) orally 1 day per week for 8 to 12 weeks, followed by
- 800 IU–2000 IU of vitamin D3 daily
Ergocalciferol is present in plant sources and fortified nutritional alternatives. Cholecalciferol is usually in fish, meat, and eggs. When using vitamin D supplements, accumulating evidence favors the use of cholecalciferol over ergocalciferol because its side chain has a higher affinity for DPB, thus conferring a longer half-life and a more potent ability to increase vitamin D levels.
Since inadequate calcium intake may contribute to the development of osteomalacia, patients should also take at least 1000 mg of calcium per day while being treated for vitamin D deficiency. This dose may need to be increased in patients with malabsorption syndromes, who may also have increased vitamin D dosing requirements. Patients with liver and renal disease might be unable to utilize vitamin D2 or D3 effectively, so calcidiol or calcitriol should be considered.[20]
Healing of osteomalacia is achieved when there are increases in urine calcium excretion and bone mineral density. Serum calcium and phosphate may normalize after a few weeks of treatment, but normalization of bone alkaline phosphatase lags, and those levels may stay elevated for months.[21]
Differential Diagnosis
Depending on the presenting symptoms, the initial differential diagnosis can be extensive. Clinical history, physical exam, laboratory values, and imaging can narrow the possibilities. However, specific diagnoses may present with similar symptoms and lab values and will require exclusion. These include metastatic disease, primary hyperparathyroidism, and renal osteodystrophy.
Osteoblastic bone metastases have similar lab findings and may also show multiple zones of uptake by bone scintigraphy. Further evaluation may be warranted to exclude malignancy. Multiple myeloma can present with similar clinical symptoms (ie, bone pain and weakness) but will often reveal lytic lesions on radiographs. Patients with multiple myeloma may also have anemia and decreased renal function.
Primary hyperparathyroidism should present with hypophosphatemia, increased bone alkaline phosphatase, and increased zones of uptake. However, it usually presents with hypercalcemia, which is atypical in osteomalacia. In renal osteodystrophy, hyperphosphatemia, rather than hypophosphatemia, is typically observed.
Prognosis
Osteomalacia is a preventable metabolic bone disorder. Most cases are related to vitamin D deficiency, so they can usually be treated appropriately and cured. If other clinical factors have contributed to the development of osteomalacia, then treatment will need to be tailored and adjusted as necessary.
Once identified and an appropriate treatment plan is in place, lab values may begin to normalize within weeks of initiation. Symptom improvement is also appreciable in a similar period. Patients will require interval lab monitoring after starting therapy. Overall, complete healing of osteomalacia may take many months to over a year, depending on the cause.
Complications
Due to poor osteoid mineralization, several complications may occur if osteomalacia is left untreated. Insufficiency fractures, also known as Looser zones, can present as bone pain and occur with little or no trauma. They are typically bilateral, perpendicular to the cortex, and usually involve the femoral neck, pubic and ischial rami. Reports also exist of Looser zones in the ribs, scapulae, and clavicles. Spinal compression fractures are less common and are usually associated with osteoporosis. Researchers have also reported kyphoscoliosis in patients with long-standing osteomalacia.[22]
Consultations
Whenever osteomalacia is suspected, the patient should be evaluated and treated by any specialty, from primary care and family medicine clinicians to endocrinologists or rheumatologists who might be seeing the patient for other bone-related diseases. Radiology can help clarify the relevant findings in plain x-rays or any other imaging studies, while orthopedic surgeons should consider osteomalacia during the checkups of patients suffering fractures. The collaboration among different medical professionals can help optimize the management of patients with diagnosed osteomalacia.
Deterrence and Patient Education
Certain populations are at greater risk for developing osteomalacia. Risk factors are as follows:
- Dark skin
- Decreased sunlight-to-skin exposure
- Diets deficient in vitamin D
- Medications that may precipitate vitamin D deficiency
- Obesity
- Older individuals
- Malabsorptive syndromes
- Renal or hepatic disease
Although insufficient data recommends obtaining serum 25(OH)D levels in asymptomatic patients, clinicians should be aware of these factors that may put their patients at risk. It is important to educate patients about these risks and, if possible, to make helpful suggestions on how to make tolerable lifestyle changes. In patients who come from more conservative cultures, a vitamin D-deficient diet, and inadequate direct sunlight exposure may get overlooked by clinicians. Foods with the highest content of naturally occurring vitamin D are usually meat or fish-based. Since patients with vegetarian diets will not consume these foods, educating them on alternative sources of vitamin D-enriched nutrition is important. These include fortified milk, yogurt, cheese, orange juice, bread, and UVB-enhanced mushrooms. The biological significance of consuming these foods requires further assessment.[23][24]
Enhancing Healthcare Team Outcomes
Patient-centered care for individuals with osteomalacia necessitates a multidisciplinary approach involving physicians, advanced care practitioners, nurses, pharmacists, and other healthcare professionals. Medical professionals should possess the clinical skills to recognize and diagnose osteomalacia. These skills include understanding the clinical manifestations, interpreting relevant laboratory results (eg, vitamin D levels), and performing bone density scans when needed. Clinicians should be skilled in designing and implementing patient-specific treatment plans, such as prescribing appropriate vitamin D supplementation, recommending dietary adjustments, and managing underlying conditions contributing to osteomalacia. A patient-centered approach involves tailoring care to individual needs, preferences, and values. Healthcare professionals should engage patients in shared decision-making, ensuring they understand their condition and treatment options. Interprofessional teams should follow evidence-based guidelines and stay updated with the latest research to provide the best care for osteomalacia patients.
The key to achieving successful results is patient education; thus, all clinicians have a vital role in preventing the high morbidity of the disorder. The interprofessional team is responsible for educating patients about the importance of vitamin D, sunlight exposure, and adherence to treatment plans to prevent recurrence.
Fortified foods are those that have been modified to include essential nutrients. In randomized controlled trials, fortified vitamin D foods, including dairy products, bread, orange juice, and UVB-enhanced mushrooms, have been shown to be effective at increasing circulating levels of 25(OH)D without adverse side effects. Most countries have individual national policies regarding food enhancement. However, current fortification levels may not satisfy physiologic requirements; this particularly applies to patients already at risk for vitamin D or calcium nutritional deficiencies. Successful enhancement of animal products has also been demonstrated in pigs, hens, and fish by utilizing vitamin D3-enriched feeding. Current results are promising, but further research is necessary on the impact of widespread introduction, particularly in developing countries. Patients need long-term follow-up as the resolution can take months. Dietitians and nurses should continue to educate patients about the importance of a healthy diet, which is also reinforced by vitamin D supplements.[25] If the treating clinician decides to supplement with exogenous vitamin D, a pharmacist should be consulted to vet the precise agent and assist with appropriate dosing for the condition.
Nurses can counsel the patient on administration and assist in monitoring and evaluating results on follow-up visits, reporting their findings and concerns to the prescriber. Close communication among interprofessional healthcare team members is vital for comprehensive care and improved patient outcomes. Physicians, nurses, pharmacists, and other healthcare providers should communicate openly, sharing insights and updates on patient progress, medication adjustments, and potential complications.
Collaborative care coordination among healthcare providers ensures that all aspects of a patient's health are considered, including comorbidities and medication interactions. Regular follow-up appointments and assessments are essential to monitor treatment efficacy, address adverse effects, and prevent complications. The interprofessional team should emphasize the importance of compliance with treatment plans and lifestyle modifications. Healthcare providers should facilitate referrals to specialists such as endocrinologists or dietitians to address complex cases or nutritional deficiencies when necessary.
By integrating these skills, strategies, and responsibilities, the interprofessional team can enhance patient-centered care, improve outcomes, ensure patient safety, and optimize team performance in managing osteomalacia. This collaborative approach is essential for addressing the multifaceted nature of the condition and achieving the best possible results for patients.