Introduction
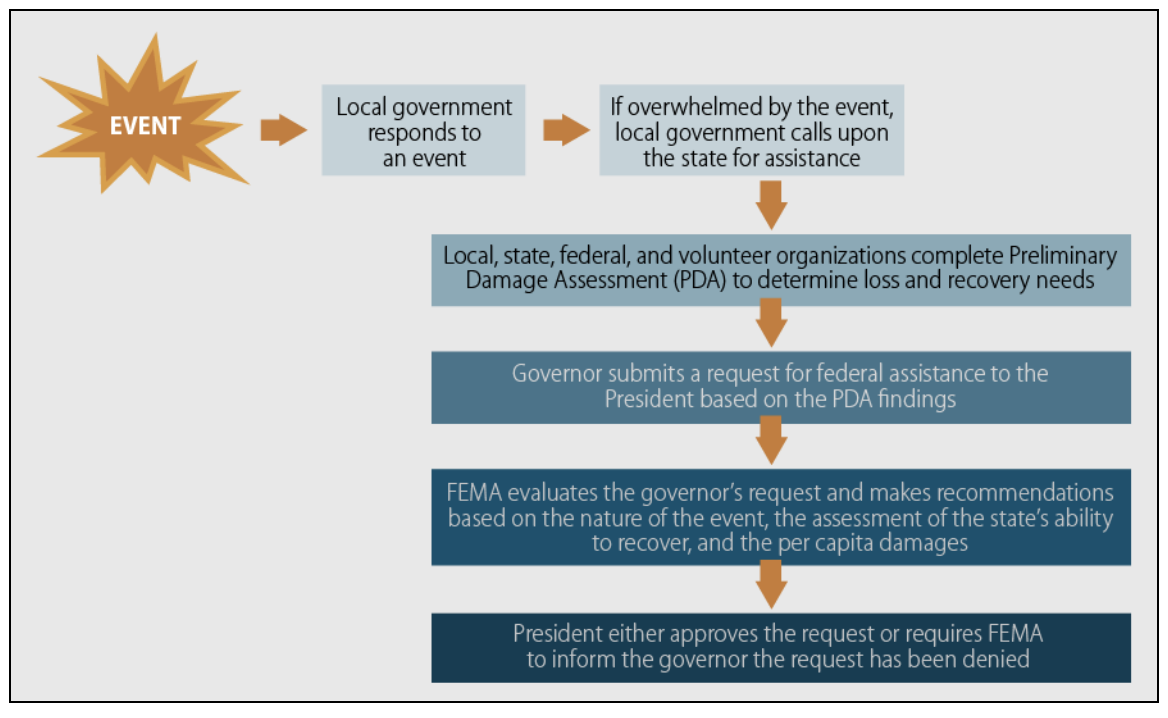
A disaster, as defined by the Federal Emergency Management Agency (FEMA), is "a non-routine event that exceeds the capacity of the affected area to respond to it in such a way as to save lives; to preserve property; and to maintain the social, ecological, economic, and political stability of the affected region." When a disaster occurs, the Stafford Act allows the state governor or tribal leader (hereafter "governor") of the affected area to petition the President of the United States for a disaster declaration, which mobilizes federal resources to augment local resources in the aftermath of the disaster. Local and state resources are expected to be able to manage the first 72 hours of an incident, after which federal resources can support and augment local efforts but not supplant them (See Image. The Stafford Act Process for Declaring Emergencies and Major Disasters).
After the Disaster
In the aftermath of a disaster, the local response includes the following:
- Providing first responder resources
- Activating the Emergency Operations Center and Comprehensive Emergency Management Plan
- Coordinating the response with local agencies
- Communicating with and submitting Situation Reports (SITREPS) to the state agency
- Utilizing regional mutual aid agreements
- Activating state and federal response agreements
- Announcing a state of emergency
- Request aid from the State Emergency Management Agency
The state's responsibility following a disaster includes evaluating SITREPS, response efforts and requests for Assistance provided by locales, activating the State Emergency Operations Center, and determining whether federal Assistance is needed. The state governor may also proclaim a "State of Emergency," which will put into motion the state disaster preparedness plan that allows for activating state resources and requests for federal resources through the Stafford Act or other applicable federal programs if needed.
Once a disaster has occurred and it is apparent that the area’s recovery needs outweigh the scope of local resources, the governor will contact their local FEMA office to request a joint federal-state and tribal preliminary damage assessment (PDA). This assessment should outline how and why the provincial government resources are inadequate to address the local disaster. In conjunction with local representatives, the federal team assesses the affected area to determine the extent of the disaster, who and what public resources are affected, and what federal Assistance will be needed. The request for disaster declaration must be made through the local FEMA office within 30 days of the disaster.
The Process of Disaster Declaration
After completing the PDA, the governor may petition the President via the regional FEMA office for a disaster declaration. Concurrently, the governor should execute the region’s emergency plan. He or she is responsible for detailing what local resources are committed to disaster relief, estimating the damage to public and private sector assets, and estimating what resources are needed under the Stafford Act.
Once federal Assistance has been approved, FEMA will activate the Federal Response Plan and assign a federal coordinating officer to lead the Emergency Response Team. This team works directly with the state coordinating officer to provide a coordinated response to local and state needs. They will also activate the Federal Response Plan, which coordinates federal agencies and the American Red Cross relief efforts. Additionally, FEMA will start a Washington-based Emergency Support Team to monitor ongoing efforts.
FEMA disaster assistance may include the following types of Assistance:
- Individual and household assistance
- Individuals and Households Program
- Crisis Counseling Program
- Disaster Case Management
- Disaster Unemployment Assistance
- Disaster Legal Services
- Disaster Supplemental Nutrition Assistance Program
- Public Assistance
- Debris removal
- Emergency protective measures
- Roads and bridges
- Water control facilities
- Buildings and equipment
- Utilities
- Parks, recreational, and other facilities
- Hazard Mitigation Assistance
- Reimburses state and local governments and nonprofit organizations for actions taken to mitigate or prevent long-term loss of life from natural hazards
Types of Disaster Declarations
There are 2 types of Disaster Declarations under the Stafford Act: Emergency Declarations and Major Disaster Declarations. They differ in the kind of disaster and scope of Assistance provided. For either type of disaster declaration, the governor must demonstrate that the prescribed emergency plan has been executed and describe the local and state resources already employed to address the disaster, as enumerated in the PDA.
Emergency Declarations are employed for any situation where federal Assistance is needed. Assistance may not exceed $5 million unless the president seeks additional approval by Congress. State or Tribal governments may request a pre-disaster declaration when there are imminently anticipated needs before the event. Under this type of declaration, the federal government may provide limited resources. There are 2 types of Assistance under this program: Public and Individual. States or Tribal Governments are not prohibited from seeking a Major Disaster Declaration if the needs of the locale exceed the resources provided by the Emergency Declaration. For an Emergency Declaration, the governor must describe other federal agency resources already utilized and how much additional federal Assistance is required.
Major Disaster Declarations can be made for any naturally occurring disaster or, regardless of cause, any damage caused by fire, explosions, or floods when it is estimated that damages will outstrip local and state resources. Relief can include public and individual emergency assistance and permanent work. For a Major Disaster Declaration, the regional leader must submit with their request the estimated cost of the disaster to the local private and public sector, estimates of how much Assistance is needed from the Stafford Act, and the governor must certify that they will comply with applicable cost-sharing requirements.