Continuing Education Activity
Acute ankle fractures can affect many different structures. Classification systems can help delineate the mechanism of injury and the structures damaged, which is vital in determining the best management modality. This activity reviews the evaluation, classification, and management of acute ankle fractures and highlights the role of an interprofessional team in collaborating to provide well-coordinated care to affected patients.
Objectives:
- State the etiology of acute ankle fractures.
- Explain how to evaluate for an acute ankle fracture.
- Explain the treatment options for acute ankle fractures.
- Employ interprofessional team strategies to enhance care delivery and improve outcomes for patients with acute ankle fractures.
Introduction
Ankle fractures are common injuries that could result from a trivial twisting injury in old frail patients up to high energy trauma in a young population. Treatment of these fractures aims to restore joint stability and alignment to reduce the risk of post-traumatic ankle arthritis.[1][2]
Anatomy of the Ankle Joint
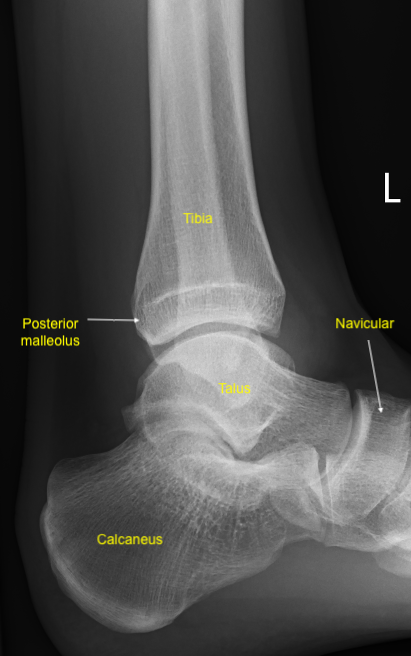
The ankle joint is a hinge synovial joint that moves in one plane to produce dorsiflexion and plantar flexion.[3] It is formed by the articulation between three bones; distal tibia, distal fibula, and talus bone. The distal tibia and fibula articular portions together form the ankle mortice, which contains the body of talus bone.[3] The ankle joint entires three malleoli; the lateral malleolus (distal end of the fibula), medial malleolus (medial lower end of the tibia), and the posterior malleolus.
Ankle joint stability is provided by the ankle mortise articulation with the talus body, the ankle syndesmosis, the ligaments and muscles around the ankle joint. The ankle syndesmosis is a fibrous joint connecting the distal tibia and fibula. The syndesmosis is formed by three main parts; the interosseous tibiofibular ligament, the anterior inferior tibiofibular ligament, and the posterior inferior tibiofibular ligament.[4] The deltoid ligament originates from the medial malleolus and attaches to the talus, navicular, and calcaneus bones and stabilizes the ankle joint against over eversion.[5] The lateral ligaments complex consists of three ligaments originating from the lateral malleolus and attaches to the talus (anterior and posterior talofibular ligaments) and the calcaneus(calcaneofibular ligament). The lateral ligament complex resists the ankle from over the inversion.[5] The ankle joint is innervated by articular branches from the tibial nerve, superficial and deep peroneal nerves. Branches from the peroneal, anterior, and posterior tibial arteries provide the arterial supply to the ankle joint.[6]
Etiology
Ankle fractures can be caused by various modes of trauma, e.g., twisting, impact, and crush injuries. Falling, tripping, or sports activities may cause twisting forces through the ankle. Impact injuries may result from falling from a height with impaction of the distal tibia and fibula against the talus. Ankle crush injury may be caused by a road traffic accident or crushing the ankle underneath a heavy object. The degree of bony comminution and soft tissue damage is directly related to the energy of trauma.
Epidemiology
About 187 per 100000 adults sustain ankle fractures every year.[7] The highest incidence in the female population is between 75 and 84 years old, compared to 15 to 24 years old for males.[8] Isolated uni malleolar fractures are the most common type accounting for 70% of the yearly incidence of all ankle fractures. About 20 % of ankle fractures are bimalleolar fractures, while trimalleolar fractures represent about 7% of all ankle fractures. Open ankle fractures incidence is about 2% of all ankle fractures.[8]
Pathophysiology
The ankle joint bony and ligamentous structures from a complete ring. Whenever the ring is broken, it happens in two places. Based on the evaluation of ankle fractures, a full assessment of the whole ankle ring is necessary to avoid missing any bony or ligamentous injury. Different systems have been developed to classify ankle fractures.
Anatomical Classification
Classifies ankle fractures depending on the anatomical location into
- Isolated medial malleolus fracture
- Isolated lateral malleolus fracture
- Bimalleolar ankle fracture; two malleoli are fractured, either the medial and lateral malleoli or less commonly the poster and lateral malleoli.
- Trimalleolar ankle fracture; the three ankle malleoli (medial, lateral, and posterior) are broken.
Danis-Weber Classification
This system categorizes ankle fractures based on distal fibula fracture line localization relative to the syndesmosis into three types:
- Weber type A; the distal fibula fracture is below the level of the syndesmosis. This type of fracture is usually stable and can be treated conservatively.
- Weber type B; the distal fibula fracture is located at the same level of the syndesmosis. Injuries of this type could be treated conservatively if it is a stable injury (no deltoid ligament injury nor syndesmotic injury). Unstable weber B fracture requires surgical fixation.
- Weber type C; the fibular fracture is located above the level of the syndesmosis. This type of fracture is usually unstable and requires surgical fixation.[9]
The Lauge-Hansen Classification
This classification depends on the foot position and the direction of the force causing the injury. This classification categorizes ankle fractures into four types. The first word of each type describes the foot position at the time of the injury and the second word describes the movement of the talus in ankle mortise relative to the tibia. When the foot is pronated, medial ligaments are stretched and prone to injury. When the foot is supinated, lateral ligaments are stretched and prone to injury.[10]
Supination-Adduction (SA)
- Distal fibula transverse fracture
- Medial malleolus vertical fracture
Supination-External Rotation (SER) - most common ankle injury (60% fractures)
- Anterior inferior tibiofibular ligament injury
- Spiral (or oblique) fracture of the distal fibula
- Posterior inferior tibiofibular ligament injury OR posterior malleolus avulsion
- Fracture of medial malleolus OR deltoid ligament injury
Pronation-External Rotation (PER)
- Fracture of medial malleolus OR deltoid ligament injury
- Anterior inferior tibiofibular ligament injury
- Spiral (or oblique) fracture of the fibula (aspect proximal to tibial plafond)
- Posterior inferior tibiofibular ligament injury OR posterior malleolus avulsion
Pronation-Abduction (PA)
- Fracture of medial malleolus OR deltoid ligament injury
- Anterior inferior tibiofibular ligament injury
- Comminuted or transverse fibular fracture (proximal to tibial plafond)
Injuries always occur in a cumulative pattern; for example, a SER4 injury includes injuries of SER1, SER2, and SER3.[10]
Other Types of Ankle Fractures
Maisonneuve Injury
It is an unstable ankle injury caused by pronation external rotation injury. Maisonneuve injury combines a proximal fibular fracture with tibiofibular syndesmosis and deltoid ligament injury with or without medial malleolus fracture. This unstable injury requires operative treatment.[11]
Pilon Fracture
This injury is the comminuted fracture of the tibial plafond (distal end of the tibia, including the articular surface). Pilon fracture usually results from high energy axial loading trauma, e.g., fall from a high distance causing impaction of the talus against the tibial plafond.[12]
Bosworth Fracture-Dislocation
This is a rare type of ankle fracture dislocation where the fibula is posteriorly dislocated. The poster tibial border blocks the fibula reduction. Therefore operative treatment is required to reduce and fix the fibula in the incisura fibularis.[13]
History and Physical
History is an integral part of any medical evaluation. The clinician needs to obtain a full history to cover all the following:
- Medical background; comorbidities including diabetes, peripheral vascular disease, peripheral neuropathy, inflammatory joint diseases, obesity, kidney diseases affect the prognosis of ankle fractures. Uncontrolled diabetes, peripheral vascular disease, peripheral neuropathic disorders affect fracture and surgical wound healing and increase the risk of Charcot's joint. If indicated, all medical and systemic diseases should be addressed and optimized prior to the surgery.
- Social history; A patient's baseline/goals should be established through social history, including the patient’s level of mobility pre-injury, home situation, and regular activities, as well as their future functional goals. Smoking and alcohol overuse can complicate wound and fracture healing.
- History of the injury; it is important to identify the mechanism of injury to understand the nature and severity of the injury. Higher energy mechanism should raise the specter of compartment syndrome of the leg or a more grave injury such as a pilon fracture (axial loading). The ankle position at the time of injury and subsequent direction of force generally dictates the fracture pattern, as described by the Lauge-Hansen classification system.
- Venous thromboembolism risk (VTE) assessment should be completed for all patients who sustain ankle fractures to identify the potential risk factors to develop deep venous thrombosis (DVT). Risk factors include but are not limited to smoking, previous DVT, family history of DVT, high Body mass index, hormonal therapy, and oral contraceptive pills. Patients who are at high risk for VTE should receive the appropriate prophylaxis treatment.
Evaluation
Clinical Assessment
1. Adult Trauma Life Support Primary and Secondary Survey
All trauma patients should be assessed according to trauma assessment principles. The primary ATLS survey should be completed in order from A to E to rule out any life-threatening injury:
- A: Airway management and cervical spine stabilization.
- B: Breathing
- C: Circulation and hamorrage control
- D: Disability to assess the neurologic status
- E: Exposure[14]
2. Neurvascualr Assement
A documented neurovascular assessment is mandatory to be performed before and after any attempt for ankle manipulation. Neurovascular assessment includes the color and temperature of the foot. Pale, cold foot indicates a critical vascular compromise. Dorsalis pedis posterior tibial pulses should be assessed and compared to the contralateral side. If there is any clinical concern for vascular compromise or skin tenting, urgent ankle reduction should be attempted immediately in an attempt to regain vascular flow followed by neurovascular reassessment s Hand doppler is a quick and non-invasive method to assess the vascular flow in the foot. Neurological assessment should include the motor and sensory function of deep peroneal, superficial peroneal, tibial, sural medial, and lateral plantar nerves.
3. Soft Tissue Assessment
Threatened skin of a deformed ankle necessitates urgent ankle reduction and splinting to reduce soft tissue stretching. Soft tissue integrity and the degree of swelling will affect the treatment choice and the timing of surgical fixation.
4. Examination of the Proximal Fibula
Examination of the proximal fibula and the knee joint is required to avoid missing any higher injury as Maisonneuve fracture injury.
Ottawa Ankle Rules
Ankle radiographs should be requested if there is pain or tenderness in either malleolus AND one of the following:
- Tenderness of the bone at the posterior edge or tip (within 6 cm) of either the lateral or medial malleolus
- Patient unable to bear weight at the time of injury AND on arrival to the emergency department. Weight-bearing is determined by the patient's ability to take four steps.[15]
Imaging Modalities
1. Plain Radiographs
X-rays are the first line of investigation to assess ankle injury. Obtaining X-rays should not delay the urgent reduction of the clinically obvious deformed ankle. Recommended X-rays views to assess ankle injuries include; anteroposterior, lateral, and Mortise views.
Anteroposterior (AP) ankle view: assess for soft tissue swelling that may lead to the discovery of other more subtle fractures
Lateral view: assess posterior malleolus, talus dome relative to the distal mortise, e.g., if it is dislocated anteriorly or posteriorly.
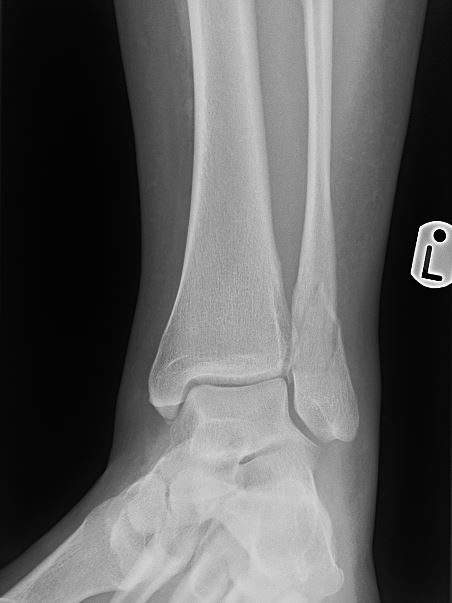
Morise view is important to assess the ankle mortise(tibial plafond , medial malleus, lateral malleolus and talar dome).[16] Mortise view is an anteroposterior ankle X-ray with the leg internally rotated 15 to 20 degrees, and the ankle is dorsiflexed. This view evaluates talus positioning and syndesmosis widening. In a normal ankle, this should show a uniform width of space through the mortise joint space.
Weight-bearing and external rotation stress views are indicated to assess fracture stability and rule out deltoid ligament and syndesmotic injury. Full tibia and fibula length X-rays are valuable to rule out proximal fibula fracture in Maisonneuve injury.
2. Computed Tomography (CT scan)
Ankle CT scan is useful to assess the articular surface, fractures configurations, and the degree of bone comminution. CT scan is usually organized for operative planning in complex ankle fractures. CT scan is also useful to assess posterior malleolar fractures.[17]
3. Magnetic Resonance Imaging (MRI) Scan
Ankle MRI is valuable to assess ligamentous injuries, e.g., deltoid ligament sprain, lateral ligament complex sprain, syndesmotic disruption, chondral lesions, and stress fractures.
Treatment / Management
Ankle fracture treatment aims to restore and stabilize the ankle mortise, which could be achieved by conservative measures in stable ankle fractures and surgical fixation in unstable ankle fractures.[18]
Non-operative Treatment
Indications
- Stable ankle fractures, e.g., isolated unimalleolar ankle fracture with no talar shift on weight-bearing ankle X-rays.
- Patient unfit for surgery or refusing surgery.
- Poor soft tissue conditions.
Non-operative Treatment
- Below knee cast
- Fracture reduction and application of a close contact cast under image guidance: could be a valid option for unstable ankle fracture in patients above 60 or who are unfit for surgery.[19]
- Walking boot
- Proper analgesia
Operative Treatment
Open Reduction and Internal Fixation (ORIF)
Urgent open reduction of ankle fracture dislocation may be required if closed reduction attempts have failed or there is a neurovascular deficit. Ankle fractures ORIF is usually indicated for patients with unstable ankle mortise who are fit for surgery and have a good soft tissue condition. Surgical fixation is usually performed either in the first 24 hours or after few days to allow soft tissue swelling to subside reduce the risk of wound dehiscence. Ankle fracture ORIF is a suitable treatment for:
- Uni malleolar fractures with talar shift on weight-bearing ankle X-rays
- Bimalleolar ankle fractures
- Trimalleolar ankle fractures
- Pilon fracture
- Maisonneuve fracture
Fibula fractures can be fixed by plate and screws or fibular nails. Fibular nails are more suitable for comminuted fractures with poor bone quality. Transverse medial malleolus fracture can be fixed by partially threaded screws or tension band wiring to allow compression at the fracture site. Vertical medical malleolus fractures require buttressing fixation by an anti-glide plate. Posterior malleolus fracture can be fixed by a posteroanterior lag screw or by an anti-glide plate. The ankle syndesmosis should be assessed intraoperatively either by performing the Hook test (Cotton test) or by obtaining intraoperative stress external rotation views.[20][21] The Hook test can be performed by the lateral distraction of the fibula by using a bone hook under the image intensifier screen. If there is >2mm displacement of the fibula, the hook test is positive.[22] If the hook test is positive and there is a syndesmosis diastasis, the syndesmosis should be reduced by applying a big reduction clamp to the medial and lateral malleoli then fixed either by syndesmotic screws or tight robes.
Spanning External Fixator
This is usually indicated as a temporary fixation method for unstable ankle fractures in case of severe soft tissue swelling or open fractures. Application of an external fixator will hold the ankle mortise in a safe position allowing the soft tissue to heal and settle. Then ankle fracture ORIF can be done in a second-stage surgery when the soft tissue is ready and can be closed safely. On application of the external fixation, the planning for surgical fixation should be considered, and pins should be inserted away from the site of the surgical approach for ankle ORIF.
Differential Diagnosis
Ankle fractures should be differentiated from other foot and ankle traumatic conditions.
Deltoid Ligament Sprain
Examination usually shows tenderness and swelling over the medial malleolus. Weight-bearing ankle X-rays may show a talar shift. MRI scan could be useful but for the diagnosis of the deltoid ligament sprain.
Lateral Collateral Complex Sprain
Examination usually shows tenderness and swelling over the medial malleolus. Weight-bearing ankle X-rays may show a talar shift. MRI scan could be useful but for the diagnosis of the lateral ligament complex sprain.
Tendon Achilles Rupture
There is usually a history of sharp pain or a feeling of a snap in the back of the affected ankle. Clinical assessment may reveal a palpable gap over the tendon Achilles and positive Simmonds test. Simmonds test should be performed in a prone position. Squeezing of the calf muscles by the examiner should move the foot to a plantarflexion position (negative Simmonds test). In tendon Achilles rupture, no foot plantar flexion will occur on squeezing the calf (positive Simmonds test). X-rays are usually negative in case of tendon Achilles rupture. Ultrasound scan is useful in the tendon Achilles rupture setting to assess the degree of rupture and length of tendon gap.
Prognosis
For patients with stable fractures that do not require operative repair, the prognosis is excellent. They can gradually bear weight and be back at baseline as early as 6 to 8 weeks after the initial injury. In those with unstable fractures that undergo ORIF, although full weight-bearing can occur as early as 6 to 8 weeks, it may take longer until full final functional results. The incidence of ankle joint post-traumatic arthritis is about 14 % of ankle fractures even with anatomical reduction and stable fixation, possibly caused by chondral injury.[23]
Complications
Complications following ankle fractures can occur after both conservative nonoperative management and operative management.[24]
Nonoperative Management Complications May Include
- Ankle stiffness
- DVT and pulmonary embolism
- Ankle mortise redislocation and requirement of a further ankle manipulation.
- Skin ulceration due to cast pressure
- Fracture delayed union
- Fracture non-union
- Fracture malunion
- Ankle chronic instability
- Delayed return to functional activity
- Ankle arthritic changes
Operative Management Complications May Include
- Infection
- Painful scar
- Wound dehiscence
- Metalwork failure (e.g., broken plate and loose screw )
- Mal positioned metal work (e.g., screw protrusion into the joint)
- Prominent screws
- Fracture non-union
- Fracture delayed union
- Nerves damage
- Vascular damage
Another complication of ankle fracture seen in people with diabetes is Charcot arthropathy, also known as neuropathic arthropathy. This condition occurs when there is a progressive degeneration of the ankle joint, which leads to the destruction of the bone, increased bone resorption, which ultimately leads to deformity. Long-term complications of this may lead to ulceration, infection, or eventual amputation.
Deterrence and Patient Education
In patients with ankle fractures, education is vital. For those with stable fractures that do not require surgical management, educating patients regarding appropriate follow-up is essential. They must receive information regarding the expected course of healing so that they can return for re-assessment when necessary or if healing delays. In those with surgical management, the importance of physical therapy and weight-bearing goals need to be discussed before the patient leaving the hospital — red flags of delayed or inadequate healing need to be discussed with all patients.
Pearls and Other Issues
- It is essential to complete the ATLS primary survey to identify and manage any life-threatening injury. This is followed by the secondary survey, including examining the affected limb.
- The examination should include the soft tissue assessment and neurovascular status.
- Ankle fracture-dislocation requires urgent manipulation to restore the ankle mortise.
- The appropriate imaging should be obtained to help the diagnosis and management.
- Always assess the neurovascular status of the ankle before and after reduction and splinting.
- There may be accessory ossicles in the joint due to anatomical variants that can be confused for an avulsion fracture in a trauma.
Enhancing Healthcare Team Outcomes
Management in the emergency department of patients presenting with ankle fractures is required a multidisciplinary approach. Patients who sustain high-energy trauma, e.g., road traffic accidents or falling from a height, require the presence of the whole trauma team and managed in a trauma call setting according to the ATLS principles. Ankle fractures should not distract the clinician from a life-threatening injury, e.g., hemothorax or internal organ damage that can be missed if ATLS primary survey was not completed. The attending trauma team should include a trauma leader, emergency department doctor, general surgery doctor, anesthesiologist, trauma doctor radiographer, and two nurses.[14]
If procedural sedation is required for reduction, team members need to communicate about the case to ensure optimal case management. In those with unstable fractures requiring operative intervention, the orthopedic team should make a timely plan for definitive fixation depending on the soft tissue status. While in the hospital, physical therapists are essential in helping patients improve their range of motion, strength, and weight-bearing abilities. Upon discharge, it is also necessary to have open communications with case managers so that patients can be discharged to rehab centers or can heal safely at home by arranging equipment (walkers, canes, etc.), home nursing, and thromboprophylaxis prescriptions. The appropriate follow-up should be arranged for the patient to be reviewed by the orthopedic and physiotherapy team.