Introduction
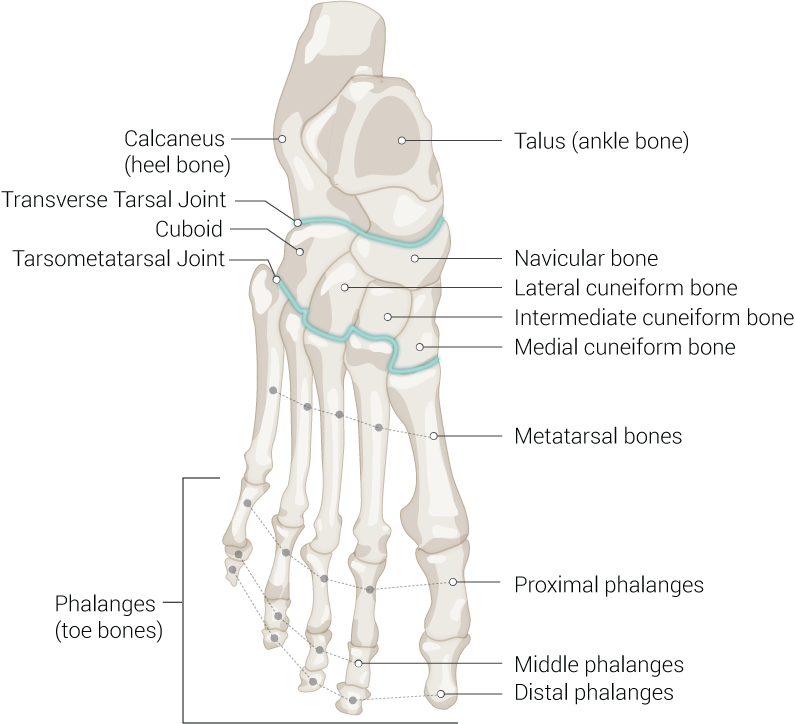
The navicular is a wedge-shaped bone that articulates with five tarsal bones (talus, cuboid, and three cuneiform bones) forming syndesmotic joints. It is located in the midfoot together with the cuboid and three cuneiform bones. Although the navicular bone is considered a small bone, it serves an essential role in building up acetabulum pedis. This bone frequently gets overlooked, but the existence of pathologies would give rise to exasperating problems. While fractures of the midfoot are an uncommon injury, one-third of human stress fractures are represented by navicular stress fractures that have a high risk of nonunion and osteonecrosis. The tibialis posterior tendon is the only tendinous insertion attached to the navicular bone and acts as the primary dynamic stabilizer of the rearfoot by preserving the medial longitudinal arch of the foot. Several ligaments also attach to the navicular bone and perform a significant function in maintaining human bipedal biomechanics.[1][2]
Structure and Function
The navicular bone has a major oblique axis that is oriented in dorsoplantar and mediolateral direction as an adaptation to the talus head that has a minus 45-degree angle of rotation. It has a round base, which is located in the dorsolateral end, and its apex is situated plantar-medially. Morphologically, the navicular bone consist of four sides (anterior, posterior, dorsal, and plantar aspect) and two ends (medial and lateral ends).[1]
Anterior Aspect
The anterior aspect of the navicular bone has a kidney-shaped appearance with its convex side on the dorsal aspect. This anterior plane divides into three articular surfaces by two slight crests that extend in a dorsoplantar direction. Overall, the anterior surface is convex; however, the articular surface division into the medial, intermediate, and lateral articular surface, generates a different direction of each articulation. The medial articular surface is the largest, is convex, and has a triangular-shaped surface. It articulates with the medial cuneiform bone. The intermediate articular surface is flat but also has a triangular shape morphology. It articulates with the intermediate or middle cuneiform bone. The lateral articular surface is the smallest among the three. It has a quadrangular surface and articulates to the lateral cuneiform bone. These three articulations converge at the plantar aspect and form the transverse tarsal arch of the foot.[1][3]
Posterior Aspect
The posterior aspect is concave and completely covered with articular cartilage. It connects with the head of the talus to form a triplanar ball-and-socket joint.[1]
Dorsal Aspect
The dorsal aspect provides insertion to various capsule-ligamentous structures. It is markedly convex with the highest point of convexity at the intermediate articular surface.[1][4]
Plantar Aspect
Similar to the dorsal aspect, the plantar aspect also provides insertion to various capsule-ligamentous structures. It is continuous medially to the navicular tuberosity and has an irregular morphology. The navicular beak often presents as an osseous prominence extending downwards, giving a quadrangular morphology of the navicular bone.[1]
Medial End
The navicular tuberosity is an osseous prominence that arises on the medial aspect of the navicular bone. It is responsible for the insertion of plantar and medial navicular ligaments, and the posterior tibial tendon as well. The accessory navicular refers to a condition where a supernumerary ossicle exists adjacent to the navicular tuberosity, giving a bony prominence on the medial side that may be symptomatic.[1]
Lateral End
The lateral end divides into two noticeable segments, which are the superior or dorsal segment and the inferior or plantar segment. While the inferior segment provides articulation to the cuboid bone, the superior segment arranges for the insertion of the medial component of the lateral calcaneonavicular ligament (bifurcate ligament).[1]
Joints and Ligaments
Acetabulum Pedis
The talocalcaneonavicular joint, also called acetabulum pedis, concurrently with the posterior talocalcaneal joint forming the subtalar articular complex. Its name comes from its similarity to the hip joint morphology and a nearly ball-and-socket resemblant function. The acetabulum pedis is made up of two basic elements, which are the osseous and ligament components. The skeletal structures included are the posterior articular surface of the navicular bone, the anterior and middle articular surface of the calcaneus that articulate with the head, and the anteromedial surface of the talus. These bones are stabilized by the plantar calcaneonavicular ligament (spring ligament) on the medial aspect and the lateral calcaneonavicular ligament (a component of the bifurcate ligament) on the lateral aspect.[5][6][7]
Plantar Calcaneonavicular Ligament
The plantar calcaneonavicular ligament, otherwise known as the spring ligament, is a group of ligaments that bond the calcaneus and the navicular to perform as a “socket” for the head of the talus. There are some controversies regarding the morphology of this ligament. While some former researchers believed that it is made up of two fascicles of fibrocartilaginous component, more current studies describe that the spring ligament is composed of two different ligaments: the superomedial and the inferior calcaneonavicular ligaments. Some recent investigators even include the talonavicular fascicle of the superficial component of the deltoid ligament as a part of the spring ligament complex.[5][8][9]
The superomedial calcaneonavicular ligament, also known as the ligamentum neglectum, is a quadrangular ligament originally considered a component of the tibiocalcaneonavicular ligament. It originates from the anteromedial margins of the sustentaculum tali which extended to the anterior margin of the calcaneal anterior articular surface. From its origin, the superomedial calcaneonavicular ligament concavely fans out in an antero-dorso-lateral direction to a broad insertion at the margin of the navicular posterior articular surface. On the dorsal aspect, it attaches to the thick fibrocartilaginous surface that performs as the base of the fibrous tunnel of the posterior tibial tendon.[5][8][9]
The inferior calcaneonavicular ligament is a trapezoidal-shaped ligament that arises from the superior portion of the coronoid fossa of os calcis, just anterior to the sustentaculum tali. Its insertion is on the lateral aspect of the navicular beak on the plantar aspect of the navicular, just lateral to the superomedial calcaneonavicular ligament insertion. The inferior calcaneonavicular ligament performs as one of the main static stabilizers of the longitudinal arch of the foot.[5][8][9]
Bifurcate Ligament
Also known as the Chopart ligament, the bifurcate ligament is a Y-shaped ligament that consists of two components that have different insertions, which are the calcaneonavicular ligament and the calcaneocuboid ligament. The proximal origin of the calcaneonavicular ligament is located at the sinus tarsi. The ligament then courses anterodorsomedially and inserts in the superior segment of the lateral end of the navicular. Two bundles of fibers form this ligament. While the superior fibers are long, resistant, and lays superficial, the inferior fibers are short and rest deep. The lateral calcaneocuboid ligament originates from the lateral side of the calcaneonavicular ligament’s origin, on the anterior aspect of the intermediary tubercle. It extends anteroinferior and attaches to the dorsal side of the cuboid. Together, these fibers form a durable band that facilitates lateral foot stabilization. [10][11] These ligaments can be injured during inversion foot and ankle injuries.
Embryology
As a distal part of the lower limb, the navicular initially emerged as a portion of a limb bud that developed within the fourth week of gestation. By the fifth week, undifferentiated mesenchymal cells migrate from the progress zone (PZ) in the process of outgrowth and become differentiated mesodermal cells. Chondrification of these mesenchymal cells started within the sixth week of gestation and reached the navicular primordial by the seventh or eighth week. The navicular is the last tarsal bone to undergo ossification; the endochondral ossification of the navicular occurs during the third year of life. The ossification center appears at the central or lateral third of the cartilaginous navicular and terminates at the medial aspect. Occasionally within the embryogenic state, the navicular bone happens to have a secondary ossification center leading to a supernumerary bone called the accessory navicular bone.[12][13]
Blood Supply and Lymphatics
The vasculature of the navicular bone primarily comes from the dorsalis pedis artery and medial plantar artery. Dorsalis pedis artery vascular branches supply blood to the dorsum of the navicular, which is divided into three to five branches when it crosses upon the dorsal aspect of the bone. The medial plantar artery is the terminal branch of the posterior tibial artery after it passes behind the medial malleolus. It is responsible for the plantar vascularization. The lateral and medial aspect, including the navicular tuberosity, receives vessels from an anastomotic network that builds up from the dorsalis pedis and the medial plantar artery. This vascular network provides a rich vascularization to the medial and lateral superficial portion of the navicular, but it lacks bone penetration causing a low level of blood supply in the central part. Increasing age results in the reduction of supplementary arteries that supply the navicular bone. It leads to a higher risk of osteonecrosis or stress fracture in the middle third of the bone.[14][15]
The lymphatic flows go along with the vasculature. It runs up the leg through the popliteal and inguinal lymph nodes, and eventually reaches the thoracic duct.[16]
Nerves
The innervation of the navicular comes from the medial plantar and deep peroneal nerves.[4]
Muscles
The tibialis posterior tendon is a solitary tendon that provides tendinous insertion in the navicular bone, which lays between the flexor digitorum longus and flexor hallucis longus muscles within the deep compartment of the leg. It converses from its broad surface on the superior aspect into a long tendon and crosses the flexor digitorum longus muscle medially at the inferior third of the leg. The posterior tibialis tendon (PTT) is located behind the medial malleolus, over the deltoid ligaments, within an osseous-fibrous groove. PTT is divided into three components at the navicular tuberosity, which are the anterior, middle, and posterior divisions. The anterior component is considered the continuation of the primary tendon because it has the largest segment. It attaches to the navicular tuberosity, the inferior capsule of the medial cuneonavicular joint, and also the inferior aspect of the medial cuneiform bone. The middle component mainly inserts into the inferior aspect of cuboid, middle cuneiform, and lateral cuneiform bones, but it also extended into the bases of the second to fifth metatarsal bones as metatarsal extensions. The posterior component gives attachment to the sustentaculum tali of the calcaneus. It performs as the main dynamic stabilizer of the rearfoot, the tibialis posterior tendon maintains the structure of the longitudinal arch of the foot. Dysfunctions of this tendon alter the biomechanics of the foot in a static and dynamic state. This problem often results in the lengthening or rupture of the spring ligament and eventually leads to the loss of the medial longitudinal arch of the foot, a condition called adult-acquired flat-foot deformity (AAFD).[17][18][19]
Physiologic Variants
Accessory Navicular Bone
The accessory navicular bone is a condition where a supernumerary ossicle presents adjacent to the navicular tuberosity on the medial side, as a result of irregular embryogenic development. Bauhin, in 1605, described it as an anatomic variant that occurs in 4 to 21% of the population. Women are more often to have this condition than men, and 50 to 90% of the cases are bilateral. It is generally visible in the radiographic examination from the age of 9 years. Most of the time, this condition was asymptomatic and occasionally diagnosed during a radiological study of the foot, however in particular circumstances, people with an accessory of the navicular could experience medial foot pain caused by injury of the fibrous connection between the navicular and its accessory, that aggravated by weight-bearing activities, walking, and running. Friction against footwear could also produce medial foot pain, especially if there is a large medial protrusion present.[20][21][22]
Accessory navicular bones got classified into three groups in 1978, according to their morphology, position, and also its connection to the navicular bone.
- Type I- also called os tibiale externum or os naviculare secundarium; it represents 30% of the total accessory type. It is considered as a 2 to 3 mm sesamoid bone with ovoid morphology, embedded within the distal part of the posterior tibial tendon.
- Type II - also known as prehallux or bifurcate hallux. This type of accessory navicular represented 50 to 60% of all types and formed due to a secondary ossification center within the navicular bone in the embryonic state. It has a triangular or heart-shaped morphology with a 12 mm length of its major axis and is connected to the navicular bone by fibrocartilage or hyaline cartilage forming a synchondrosis joint.
- Type III - also known as a cornuated navicular; it has a prominent navicular tuberosity and is considered a result of a fusion of type II.[20][23][20]
Conservative treatment, such as immobilization and anti-inflammatory medication, has often been adequate since it is commonly asymptomatic and only produces a mild grade of pain. However, in some cases of recurrent symptomatic issues and failure of conservative treatment, then a bony excision with an anatomic repair of the posterior tibial tendon might be necessary.[24][25]
Surgical Considerations
Adult Acquired Flatfoot Deformity (AAFD)
When conservative treatments failed to improve AAFD, various surgical interventions merit consideration. Medial displacement osteotomy of the calcaneus with posterior tibial tendon replacement using the flexor digitorum longus tendon, spring ligament reconstruction, subtalar arthrodesis, and triple arthrodesis are alternatives for surgical procedures to correct the flatfoot deformity.[26][27]
Navicular Fracture
Navicular fracture typically requires surgical intervention if it is an acute traumatic injury or a stress fracture that happens in high functional demand such as in athletes. The common operative procedure is an open reduction with internal fixation with the primary goal to achieve anatomical reduction and also to restore the medial column length. Surgical management often results in a satisfactory prognosis; in a case study of ten patients who underwent surgical management after suffering from a comminuted navicular fracture, achieve union with none requiring an arthrodesis. Several potential complications are avascular necrosis, malunion, nonunion, and persistent stiffness. Osteonecrosis is commonly treated with a fusion of the talonavicular or naviculocuneiform joints to restore its length and alignment.[2][15]
Clinical Significance
Adult Acquired Flatfoot Deformity
Adult acquired flatfoot deformity (AAFD) most commonly results from a posterior tibial tendon dysfunction. This failure of the posterior tibial tendon leads to an inversion of the rearfoot that blocks the Chopart joint during the middle and late phases of the gait. Therefore, the triceps surae force of contraction inserts mainly on the talonavicular joint instead of the metatarsal heads. This condition causes the head of the talus to repeatedly act on the spring ligament that results in the lengthening of the ligament, and eventually generates the AAFD. Several potential causes that lead to a dysfunction of the posterior tibial tendon include acute trauma, impingement, compression by flexor retinaculum, an accessory of the navicular bone, hypovascularization of the tendon, arthritis, chronic mechanical load, and corticosteroid injection.[26][28]
Navicular Fracture
While midfoot fractures are considered an uncommon injury, navicular stress fracture represents one-third of all stress fractures in the human body. Navicular fracture commonly happens as a consequence of either an acute traumatic injury or chronic overuse, due to high functional demands. It has a higher incidence in young individuals and athletes due to their repetitive high-force activities that make them susceptible to high-energy trauma and also musculoskeletal overuse. The Sangeorzan classification has been in wide use since its publication in 1989, for a grading system of navicular fracture. Patients with navicular fractures typically experienced pain in the midfoot area that could be associated with an inflammatory process. The navicular stress fracture could mostly be managed nonsurgically by immobilization and protected weight-bearing for a six to eight weeks period. However, in an athlete with a high functioning demand, operative intervention to repair by open reduction and internal fixation become a beneficial option. On the other hand, traumatic navicular fracture typically requires surgical intervention, especially if a displaced navicular body fracture occurred. Conservative treatment using a short-leg cast could become an option if the traumatic fracture is undisplaced or in the form of a small avulsion fracture.[15]
Kohler Disease
Kohler disease is avascular necrosis (osteonecrosis) of the navicular bone that occurs in young children most commonly within 4 to 7 years old. This condition occurs more commonly in boys and can appear bilaterally. The navicular bone is the last bone in the foot to ossify, which occurs around the third year of life; therefore, the increasing weight of the child makes the navicular bone susceptible to compression by the talus and cuneiform bones during activity. The lack of vascularization in the central third portion of the navicular increases the vulnerability to this disease. Radiology examination often shows sclerosis, fragmentation, or flattening of the navicular bone. Since Kohler disease is a self-limiting condition, surgical intervention is rarely necessary. Anti-inflammatory medication and immobilization with a short leg walking cast often bring satisfying clinical outcomes.[29][30]
Mueller-Weiss Syndrome
Mueller-Weiss syndrome (MWS), also known as Brailsford disease, is a rare disease that refers to a multifactorial spontaneous tarsal navicular osteonecrosis. Differ from Kohler disease pathology, MWS occurs in adults with the highest prevalence between 40 to 60 years of age. It is more common in women and frequently bilateral. Despite being idiopathic, some theories support the pathogenesis of MWS, including osteochondrosis, trauma, biomechanic alteration, migration of the accessory cuboid, dysplasia, and also congenital causes. The pathogenesis of MWS is considered multifactorial and related to a chronic overload to the lateral aspect of the navicular bone that is suboptimal ossified. Plain radiograph examination shows a comma-shaped deformity of the navicular bone, caused by the collapse on the lateral aspect. Non-operative treatment such as anti-inflammatory medications, orthotics, and immobilization by short-leg cast, should be attempted before considering surgical intervention. If symptoms persist after conservative treatment, then surgery may be indicated to relieve pain and to restore the plantar and medial longitudinal arch. Talonaviculocuneiform arthrodesis with bone grafting often gives a satisfying result. Other surgical procedures include the percutaneous core decompression of the navicular bone, isolated talonavicular arthrodesis, and also triple arthrodesis (fusion of the subtalar, talonavicular, and calcaneocuboid joints).[31][32][33]
Other Issues
Talonavicular Ligament Injury
Acute ankle injury is one of the leading causes of emergency department attendance; however, talonavicular ligament (TNL) injuries often remain unnoticed compared to the other ligaments causing ankle injuries (lateral ligamentous complex, anterior talofibular ligament, and calcaneofibular ligament). In 2016, a study conducted by Dea showed that TNL injury is surprisingly common, with a prevalence of 21% when someone experienced an acute ankle sprain. To date, the proven consequences of TNL injury remain unknown, but the suspicion is that the damage could alter the biomechanics of the foot and eventually leads to degenerative changes that most likely require surgical interventions.[34]
Tarsal Coalition
Tarsal coalition is a condition of fused tarsal bones that leads to a rigid flat foot and foot pain. This condition resulted from an embryology anomaly caused by the failure of mesenchymal segmentation and development of fibrous, cartilage, or bone, forming coalitions of the tarsal bones. 50% of the case happens bilaterally, and 20% are multiple coalitions. Calcaneonavicular coalition is the most common type, while talocalcaneal and talonavicular types are much less common. The talonavicular coalition only represents 1% of all tarsal coalition. An elongated anterior process of the calcaneus, also known as the anteater sign, is a classic radiology indication of a calcaneonavicular coalition. Non-operative management includes anti-inflammatories, activity modification, and immobilization by a cast. Surgical intervention could be an option if conservative treatments did not meet a satisfying outcome. Coalition resection with interposition graft relieves the pain in most tarsal coalition cases. Subtalar arthrodesis and triple arthrodesis are indicated in more severe cases.[35][36][37]