Introduction
The genioglossus is a paired tongue muscle that is in the group of extrinsic muscles of the tongue. The other extrinsic muscles of the tongue are the hyoglossus (chondroglossus), styloglossus and the palatoglossus.[1][1] All of these extrinsic muscles are within proximity of one another, which is why the entirety of the extrinsic muscle group usually functions as a unit. Each muscle has its individual function, but there tends to be more than one extrinsic muscle functioning at the same time.
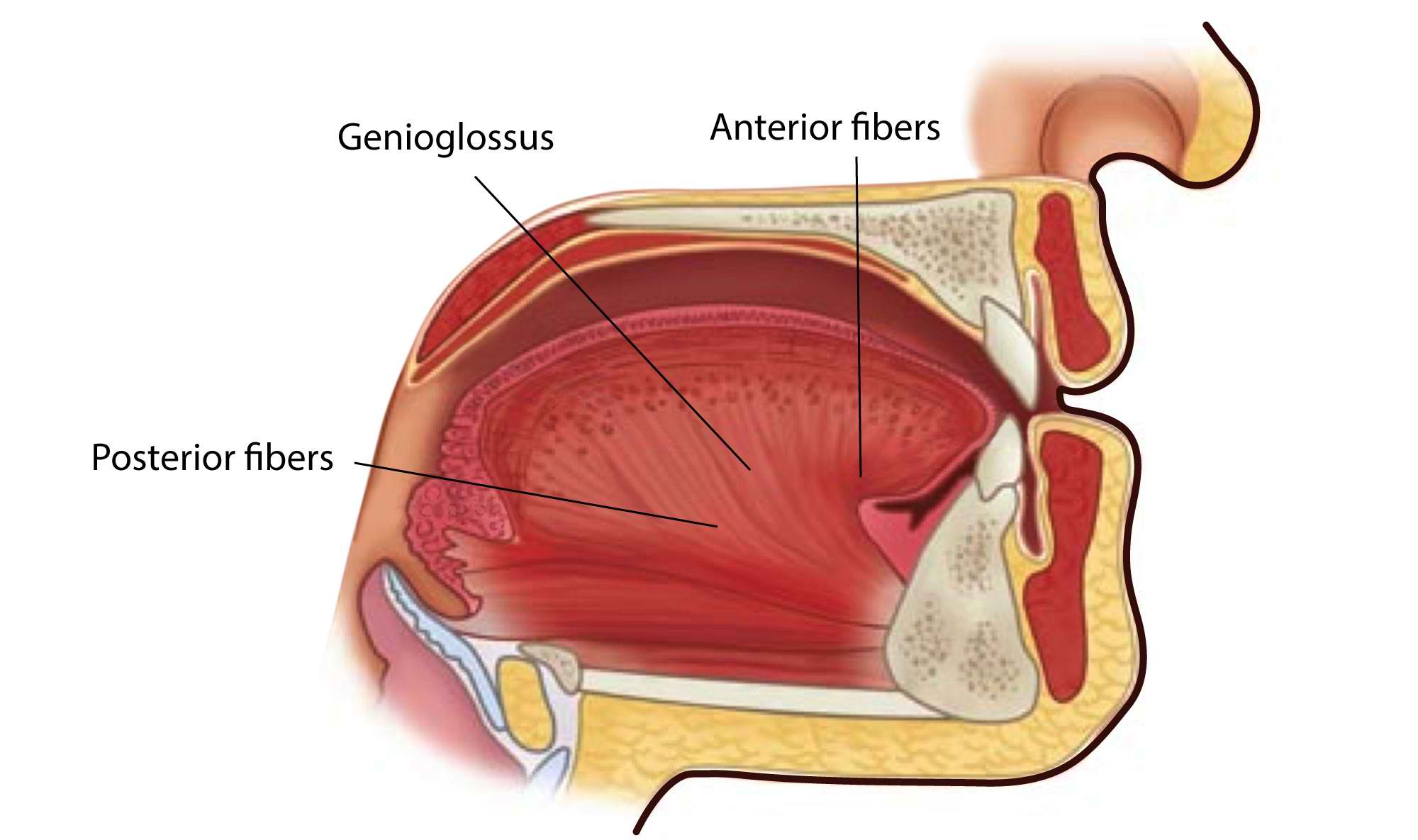
Histologically the genioglossus muscle has significant type 2 fibers present in the anterior section of the genioglossus muscle, whereas the posterior portion of the muscles does not have a large portion of type 2 fibers present. The specific fibers present in the particular portion of the genioglossus muscle determine the function of the muscle. For example, the anterior portion of the genioglossus contains type 2 fibers, and this suggests that this portion of the genioglossus muscle participates in phasic action.[2] The posterior portion while it does not contain many type 2 fibers has significant muscle strength compared to the anterior portion of the genioglossus; because of this, it there are sugggestions that the posterior portion of the genioglossus holds responsibility in the nasopharyngeal airway, as well as in the production of the sound of vowels.[2][3][4]
Structure and Function
The genioglossus muscle is a fan-shaped muscle that is involved in forming most of the tongue mass. It emerges from the superior mental spines and inserts on the hyoid bone as well as the inferior portion of the tongue.[1] The genioglossus muscle divides into four main parts:
- Anterior
- Posterior
- Middle
- Inferior
These portions are separated by the macro fibers that form bundles of muscular fibers.[2][3][4]
The primary function of the genioglossus muscle is to protrude the tongue anteriorly and deviate the tongue to the opposite side.[5] It also aids in swallowing as it will create a passage to the GIT.[5] When the left and right genioglossus muscles act together, they will depress the middle part of the tongue.[6] Specific parts of the genioglossus muscle are responsible for each of these important functions; for example the anterior bundle of the genioglossus muscle is the portion of the muscle that is directly involved in protrusion of the tongue in the down and forward direction, whereas the inferior and posterior aspect of the muscle is responsible for moving the base of the tongue forward and elevating the core portion of the tongue as well.[3][4][6] The middle part of the muscle is specifically responsible for allowing the tongue to leave the oral cavity and protrude outwards.[3][4][6] When all of these specific areas of the genioglossus tongue act cohesively with one another, then the functions above can be completed.
The muscle itself also plays an essential role in both enlarging and stabilizing the upper portion of the respiratory tract, this specific section of the upper respiratory tract is very susceptible to involuntary collapse, which is why this muscle is so involved in sleep apnea patients.[5]
The genioglossus muscle can influence the hyoid bone; the muscle size can affect the function of the temporomandibular joint. The muscle is electrically involved in the generation of maximal sniff nasal inspiratory (with higher values of electromyography) and nasal expiratory pressures.
Muscle contributes to the ability to express phonemes.
Embryology
The tongue evolves from all of the pharyngeal arches; each arch is important for different aspects and functions required for the proper functioning of the tongue. The cells of the muscles of the tongue are from the embryonic origin of the myoblasts that comes from the somites of the mesoderm.[1]
The connective tissue of the muscle derives from the ectodermal leaflet.
From an embryological point of view, there is a close relationship between the genioglossus, the base of the skull (occipital bone), and the hyoid bone.
Blood Supply and Lymphatics
The genioglossus muscles are supplied blood by the external carotid artery indirectly. Their specific source is the sublingual branch of the lingual artery, which directly comes off of the external carotid artery.[1] The lingual artery is in the anterior portion of the hyoglossus where it then travels between the mylohyoid and genioglossus muscles, eventually reaching the sublingual gland.[1]
Nerves
The genioglossus muscle under the control of multiple reflexes evoked by mechanoreceptors involved in the upper respiratory tract airway.[7] The tongue has five different means of innervation all of which include; the trigeminal nerve specifically the lingual nerve, the facial nerve specifically the chorda tympani branch, the glossopharyngeal nerve, and the hypoglossal nerve.[7][8] The vagus nerve is involved in the innervation of the genioglossus.
The hypoglossal nerve also referred to as cranial nerve XII, is responsible for the innervation of both the intrinsic and extrinsic muscles; this includes the genioglossus muscles as they are part of the extrinsic muscle group.
Pleural receptors, when called upon (during an inhalation), send inhibitory afferents to the XII nucleus, to make the genioglossus muscle more able to retract and better dilate the upper airway.
Muscles
The extrinsic muscles, of which the genioglossus muscle is part of it, determine the movement of the tongue, while the intrinsic muscles determine the shape of the tongue.
Checking the shape of the tongue and its movement can give many clinical signals during the evaluation.
The ability to lower the tongue correctly allows better use of the vocal cords, for example, when using a wind instrument (clarinet).The color of the tongue requires evaluation. According to recent studies, for example, a yellow or bluish tongue may indicate the presence of type II diabetes mellitus.
The genioglossus muscle will be negatively affected by the presence of pathologies, both of the oral cavity, and systemic diseases. For example, constant hypoxia (during sleep) can alter muscle metabolism. Type 17 microRNAs (miRNAs-17) helps the genioglossus muscle satellite cells repair muscle tissue and maintain an efficient mitochondrial membrane potential. Overnight hypoxia due to airway obstruction (COPD or OSAS, or CHF) causes a decline in miRNAs-17, leading to functional muscle weakness.
Physiologic Variants
There are multiple physiological variants associated with the genioglossus muscle, one being food manipulation. The tongue is required to manipulate food around the mouth; the movement of the food within the mouth is necessary to form what is called a bolus. The bolus is what is swallowed and consumed for digestion later by the stomach. To swallow the bolus, the tongue must elevate and push posteriorly to ensure the bolus makes it past the tonsils.[9][10] In some people, the genioglossus muscle is shorter than others, and this causes difficulty swallowing as the tongue is unable to elevate entirely and push the food posteriorly.[9][11] This issue can lead to food that does not form a bolus for swallowing, which could lead to choking if the food is large enough.[12]
As stated above, some people have different length genioglossus, and if the genioglossus develops but does not develop properly and is shorter, than it should be, this can lead to speech problems. The tongue is unable to elevate or protrude, and this makes it difficult for people who suffer from this to pronounce certain words that contain the letter S in them.[10] The common tern for this condition is a lisp. There is not a surgical fix for this, and most people who suffer from this will go their whole lives with this speech abnormality.
Surgical Considerations
A hemiglossectomy is normally completed on the lateral portion of the tongue because most cancers present in that area. The lateral portion of the tongue, if oral cancer is present, will most likely be surgically resected; this surgical resection commonly affects and inhibits the proper functioning of the tongue muscles; including the genioglossus.[12] The surgeon removes the anterior and the middle portions of the genioglossus muscles during this resection as well as other intrinsic and extrinsic tongue muscles, but the posterior portion of the muscle is only minimally affected during resection. This condition makes it difficult for patients who undergo this surgery to swallow as the genioglossus muscle functions improperly due to the resection of the anterior and middle portions of the muscle.[12][13][14]
Genioglossus muscle advancement is a surgical approach in patients with obstructive sleep apnoea syndrome so that the tongue has difficulty remaining in a posterior position during sleep.
Clinical Significance
The genioglossus is a muscle responsible for airway dilation. When the muscle has decreased function, it can lead to airway constriction/obstruction.[15] This situation becomes important during sleep as a patient will have multiple airway collapses while sleeping, leading to hypoxemia during sleep, which has shown to increase the risks of strokes and sudden cardiac death.[15] How this occurs is that during REM (rapid eye movement) sleep the genioglossus muscle tends to relax and it is during this relation that the obstructive sleep apnea can occur as the muscle is no longer participating in airway dilation making the airway more prone to constriction/obstruction.[16] The way to resolve this problem is for patients who suffer from this to use a continuous positive airway pressure, also known as a CPAP while sleeping, which will allow for constant airway dilation and prevention of obstructive sleep apnea.[15] The obstructive sleep apnea has commonly been shown to occur following a uvulopalatopharyngoplasty, also referred to as a UPPP.[17]
Another clinical significance of the genioglossus muscle is that it can help test the functioning of the hypoglossal nerve. The patient will be asked by a physician to stick out their tongue. Damage to the hypoglossal nerve will cause the tongue to deviate to the side of the neural lesion, allowing the physician to know which peripheral portion of the hypoglossal nerve is damaged, right or the left.
Other Issues
Myofunctional therapy is essential for restoring the function of the genioglossus muscle after surgery or trauma or nerve injury.
The literature shows that a cervical trauma (whiplash) can negatively influence the function of the tongue and osteopathic treatment can restore the lingual function.
To assess the tension and tone of the tongue, it is possible to use a glove and a gauze and to pull the tongue out (passive protrusion), or put a finger to the side, above and below the tongue when it is protracted, to check its strength and any compensations (with the neck, eyes, or the jaw).