Continuing Education Activity
Modern society emphasizes attractiveness. A well-balanced smile plays a crucial role in self-esteem and social integration. Excessive gingival display, also known as "gummy smile," overexposes the maxillary gingiva while smiling. In some severe cases, the overexposure of the gingival tissue is evident even in the resting position of the lips. The condition is multifactorial in etiology, and more than one factor can present simultaneously. Professionals must accurately identify the cause of a gummy smile since the treatment differs according to the etiology. This activity reviews the evaluation and management of excessive gingival display and explains the role of the interprofessional team in managing patients with this condition.
Objectives:
- Describe the etiologies of the excessive gingival display, including short upper lip length, hypermobile upper lip, altered passive eruption, vertical maxillary excess (VME), dentoalveolar extrusion, and gingival hyperplasia.
- Explain the examination steps of a patient with excessive gingival display.
- Review the less invasive treatment options to address excessive gingival display.
- Review the surgical management of excessive gingival display.
Introduction
Exposing the gingiva when smiling up to some extent provides a youthful look and is cosmetically appealing.[1] A gingival display of 1 to 2 mm when smiling is considered normal.[2] Excessive gingival display, also known as "gummy smile," is the overexposure of the maxillary gingiva while smiling. In some severe cases, the overexposure of the gingival tissue is evident even in the resting position of the lips.[1]
The critical element in managing a gummy smile is identifying its etiology, which determines the treatment plan and outcomes. A gummy smile may result from various disorders, including a short or hypermobile upper lip, altered passive eruption, vertical maxillary excess (VME), dentoalveolar extrusion, and gingival hyperplasia, but VME is one of its most common causes.[3] The investigations needed to diagnose a gummy smile, and its etiology include frontal and lateral facial analysis, static and dynamic lip analysis, lip line, interlabial distance and display of incisors at rest, and complete periodontal examination. Oral radiographs and cephalometric analysis may also be needed; the latter indicated for diagnosing VME.[1]
Etiology
A gummy smile is multifactorial in etiology, and more than one factor can present simultaneously. Professionals must accurately identify the cause of the condition since the treatment differs according to the etiology.[3][4]
- Short upper lip length
- Hypermobile upper lip
- Altered passive eruption
- Gingival hyperplasia
- Vertical maxillary excess (VME)
- Dentoalveolar extrusion
Vertical Maxillary Excess (VME)
Vertical maxillary excess is the overgrowth of the maxillary bone in the vertical plane that gives an elongated appearance to the lower half of the face.[1] It is one of the most common causes of excessive gingival display, and a cephalometric analysis is usually needed to confirm its diagnosis.[1][3]
Excessive gingival display results from an occlusal plane that is lower than expected. The lower lip covering the incisal edges of the upper canines and premolars is almost a pathognomonic feature of the disorder. In VME, the anterior occlusal plane continues without interruption with the posterior occlusal plane, which differs from the overeruption of incisors.[1] Even though the upper lip appears clinically short, its length is usually normal.[1]
Altered Passive Eruption
Teeth erupt in an active phase, where the tooth reaches its occlusal position, and a passive phase, where the gingival tissues migrate apically, exposing the crown.[5] Passive eruption develops in four stages: 1) junctional epithelium on the enamel, 2) junctional epithelium in part on enamel and cementum apical to the cementoenamel junction (CEJ), 3) junctional epithelium entirely on cementum and the sulcus' base at the CEJ, 4) stage 3 and a part of the root clinically exposed.[3]
Altered passive eruption is the gingival tissue's incapacity to migrate apically past stage 2.[5] Teeth will appear short and square because the gingival tissues are coronal to the CEJ.[1]
Vital elements to diagnosing altered passive eruption include ruling out a hypermobile lip and checking the CEJ and alveolar crest location. The lips should be examined while resting and smiling. In a hyperactive lip, a translational movement from rest can be up to 10 mm, while in a normal lip activity, between 6 and 8 mm.[5] In altered passive eruption, the CEJ can be found at up to 10 mm apical to the free gingival margin.[5]
The alveolar crest level is the same as in a healthy condition: at the level of 1 to 2 mm apical to the CEJ.[5] Probing to bone and a parallel x-ray determine the alveolar crest level.[6][7][8]
Anterior Dentoalveolar Extrusion
Anterior dentoalveolar extrusion is the overeruption of the maxillary incisors, resulting in excessive gingival display due to a more coronal position of the gingival margins.[1] Tooth wear and anterior deep bite may be the causes of the anterior extrusion. A compensatory incisor overeruption is seen in cases of anterior tooth wear.[1] A discrepancy between the anterior and posterior occlusal planes is usually found in deep bite cases.[1]
Epidemiology
Around 10% of the population between 20 and 30 years of age present excessive gingival display, which is more prevalent in women.[9][10]The prevalence of the condition decreases with age due to the dropping of the upper and lower lips, which reduces the exposure of the gingiva and maxillary incisors.[11]
History and Physical
Pleasing smiles are found to show: at least the second premolars, little upper gingiva, no gingival recession with healthy interdental papillae filling all interdental areas;[12] a lower lip line that is parallel to the incisal line of the upper teeth and to a virtual line that connects the contact points of these teeth, the symmetry between anterior and posterior teeth, and teeth with correct form, position, color, and shade.[12][1]
Some authors define a gummy smile as more than 3 to 4 mm of exposed gingival tissue in a smile, whereas others consider more than 2 mm of gingival exposure as excessive.[13] In general, a gum to lip distance of 4 mm or more during a smile is deemed as "unattractive" by dentists.[14] Once we identify that a patient has excessive gingival exposure, the next step is to determine its etiology (Table 1).
| Lips |
Teeth |
Maxillary bone |
Gingiva |
| Short lip |
Dentoalveolar extrusion |
Vertical maxillary excess (VME) |
Gingival hyperplasia |
| Hypermobile lip |
Altered passive eruption |
|
|
Table 1. Etiology of excessive gingival display organized according to the affected tissue.
Evaluation
Medical History
The patient’s age indicates the dentition’s eruptive stage, which helps to identify an altered passive eruption. Gingival hyperplasia may be seen in patients taking anticonvulsants, calcium channels blockers, or immunosuppressive drugs after organ transplant.
Facial Analysis
The face must be evaluated in the frontal and lateral plane to identify any anomalies or vertical maxillary excess.[3] Most patients with VME have a skeletal class 2 relationship.[3]
Lip Analysis (static and dynamic)
When the cause of the gummy smile is in the lips, it can come from a short lip, a hypermobile lip, or both.[5]
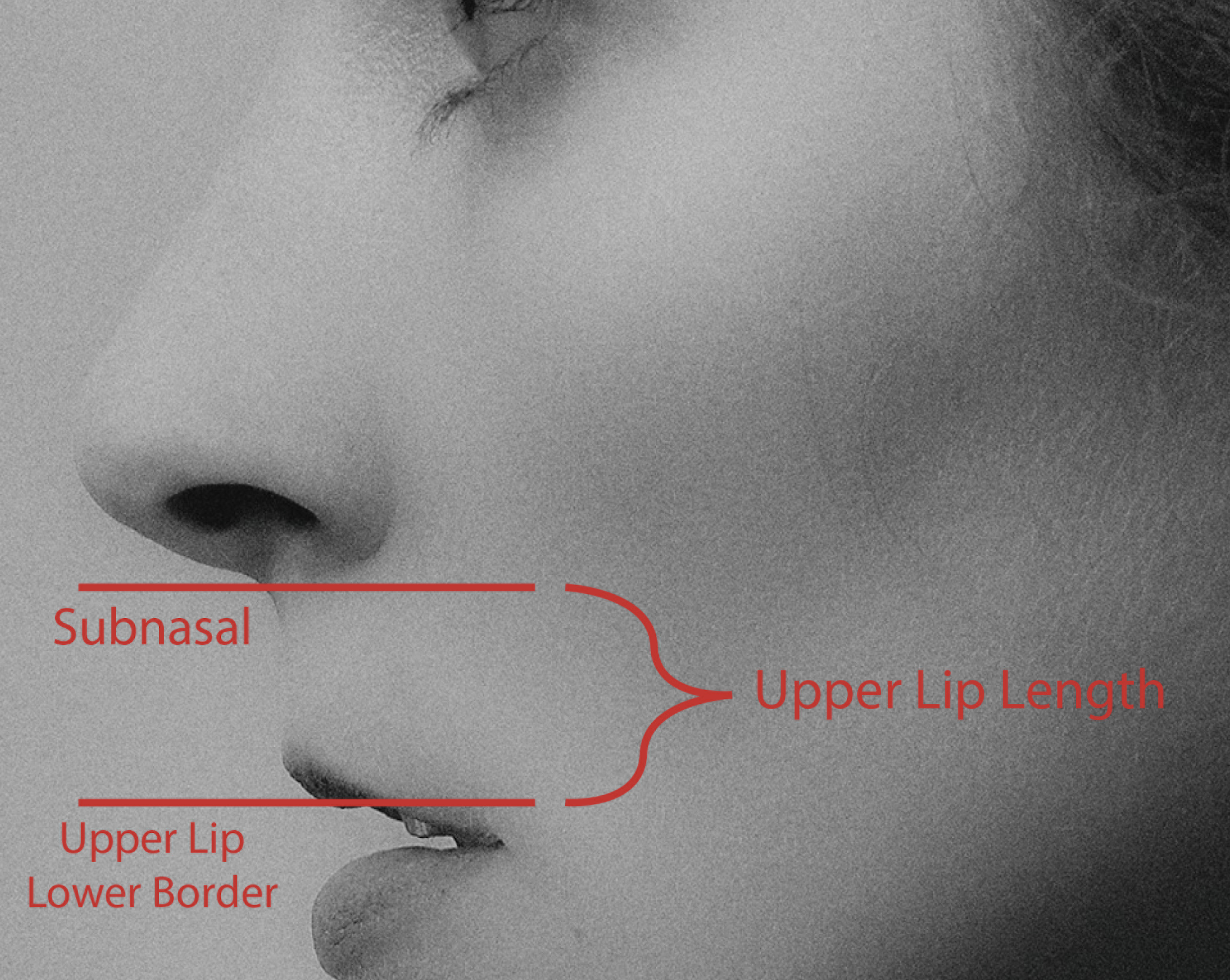
The upper lip length corresponds to the distance between the subnasale to the upper lip stomion (lower border of the upper lip). The average length is 20 to 24 mm in young adults and rises with age.[6] A measure less than 20 mm is considered a short lip, and gummy smile and lip incompetence may also be seen in such patients.[5]
A hypermobile lip (also known as hyperactive lip) results from increased activity of the upper lip elevator muscles when smiling.[1] More specifically, the hyperactivity of the levator labii superioris muscles increases the exposure of the teeth and gingival tissues when smiling due to a higher lip position, resulting in a gummy smile.[3]
Display of the Upper Central Incisors at Rest
It must be 3 to 4 mm for young women and 2 mm for young men; however, it decreases with age.[11]
Interlabial Distance at Rest
The normal interlabial distance at rest ranges from 0 to 4 mm.[3] An increased interlabial gap can be caused by short lips, dentoalveolar extrusion, or VME, and clinicians should investigate and identify which one is the cause of the discrepancy.[3][5]
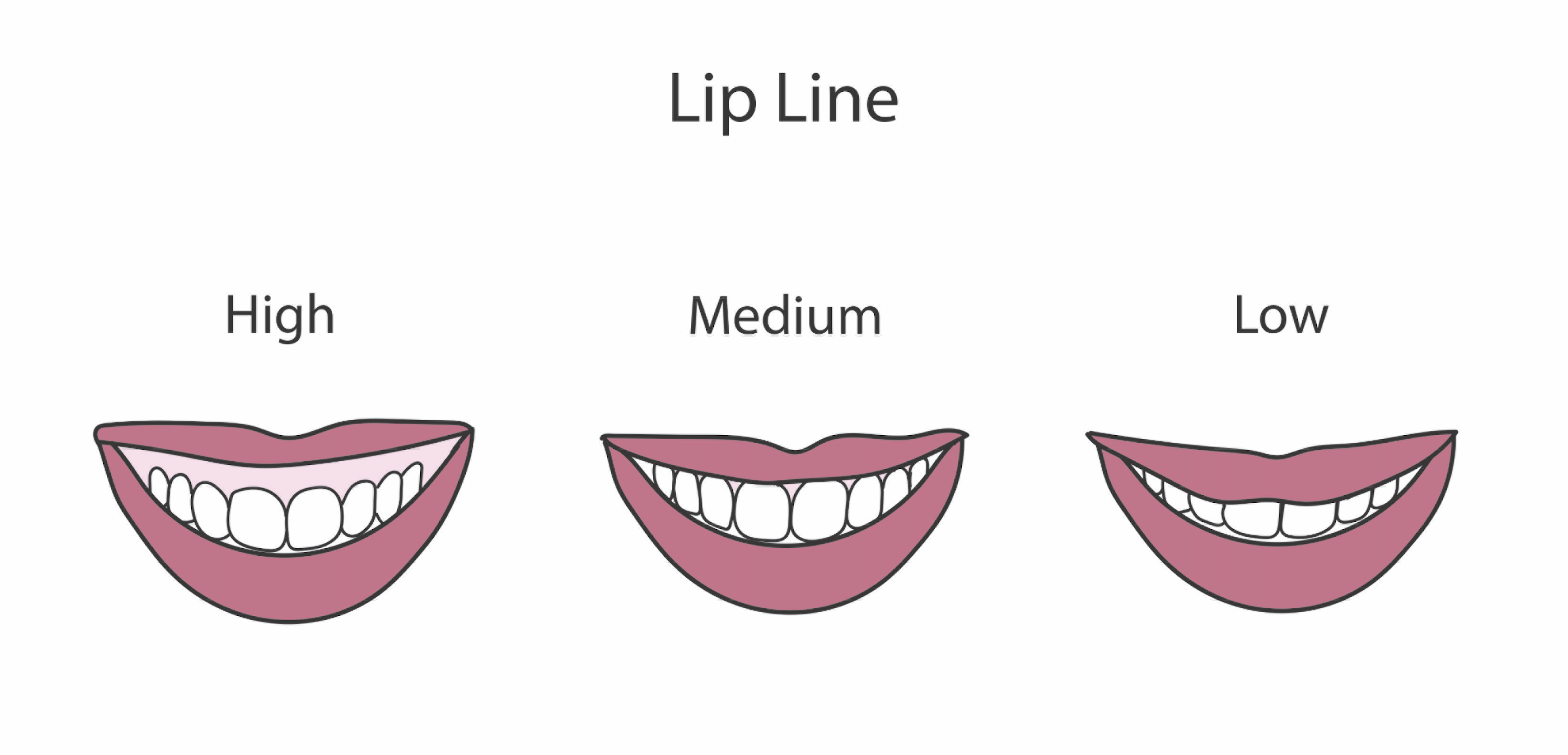
Smile Line
The smile line is defined as the upper lip position concerning the upper incisors and gingiva during a natural full smile.[9] A standard smile line shows 75% to 100% of the crowns with the interproximal gingiva.[1] A low smile line shows less than 75% of the crown – usually a male feature.[15] A high smile line (gummy smile) shows the whole crown and an excessive amount of gingiva – usually a female characteristic.[1][15]
Periodontal Examination
The periodontal examination includes measuring the width and thickness of the attached gingiva, the clinical and attachment level, the crestal bone level concerning the CEJ, and probing depths.[1] A clinical short tooth can be due to gingivitis, gingival hyperplasia, altered passive eruption, or tooth wear, and examining the periodontal tissues helps identify the etiology.[5]
Treatment / Management
- Hyaluronic acid
- Botulin toxin
- Modified lip repositioning
- Gingivectomy
- Orthodontic treatment
- Orthognathic surgery
The treatment modalities vary according to the etiology of the gummy smile - the key is accurately recognizing the cause of the pathology. In some cases, the gummy smile results from more than one factor, e.g., vertical maxillary excess and hypermobile lip, and a combination of techniques can be implemented. Less invasive treatment options include botulin toxin injection and a newer alternative: hyaluronic acid injection; the surgical management ranges from gingivectomy, modified lip repositioning, and orthognathic surgery, which is reserved for severe VME as it carries high rates of morbidity and requires hospitalization.[16] Finally, orthodontic treatment by itself may be sufficient to resolve some cases of a gummy smile.
Gingivectomy
Crown lengthening with or without bony resection, called gingivectomy, removes the excessive gingival tissue and reinsert the attachment apparatus.[16]
The decision of performing only gingivectomy or gingivectomy with osseous resection depends on the amount of biological width. A gingivectomy is sufficient to resolve a gummy smile when there are adequate osseous levels and attached gingiva, and the gingival tissue from bone to gingival crest is more than 3 mm.[16] But, a full-thickness periodontal flap in combination with osteotomy is indicated when the osseous level is near the cementoenamel junction - a gingivectomy alone will disrupt the biologic width.[17]
Lip Repositioning Surgery
Lip repositioning surgery aims at narrowing the vestibule and reducing the gingival display by restricting the muscle pull.[18] It involves eliminating a long piece of mucosa from the labial vestibule and making a partial-thickness flap between the mucogingival junction and the upper lip muscles.[17] After this, the lip mucosa is sutured to the mucogingival line.[18]
Lip repositioning surgery is indicated in mild VME and upper hypermobile lip.[5] A short upper lip of non-skeletal origin may also be addressed by repositioning.[4] It must be avoided in patients with severe VME and those with insufficient attached gingiva width.[4] The technique can be performed by electrocautery, laser, or using a scalpel.[5]
Hyaluronic Acid Infiltration
In 2018, Diaspro et al.[4] proposed what they called "a novel corrective technique" to address the concern of excessive gingival display. The procedure involves injecting a small bolus of hyaluronic acid into the paranasal region to compress the lateral fibers of the levator labii superioris alaeque nasi (LLSAN), which inhibits the motility of its deep portion.[4] This will lessen the elevation of the upper lip when smiling, significantly improving a gummy smile.[4]
The infiltration point corresponds to the most cranial part of the nasolabial fold, at around 3 mm lateral to the wing of the alar cartilage (the same anatomical site where it is commonly recommended to inject botulin toxin).[4]
Hyaluronic acid infiltration is a valid technique that can be an alternative to botulin toxin injection, although it is not appropriate for all cases of excessive gingival display.[4] It requires an experienced injector with a vast knowledge of anatomy since the substance is infiltrated in a vascularly rich zone.[4]
Botulin Toxin A Injection
Botulin toxin induces muscle paralysis by inhibiting the presynaptic release of acetylcholine at the neuromuscular junction.[5] It is a good alternative to address a gummy smile caused by a hyperactive lip.[5]
The toxin infiltrates into the levator labii superioris alaque nasi (LLSAN) muscles and levator labii superioris on both sides of the face.[19] Around 4 to 6 units of botulin toxin are injected into the following points bilaterally: 2 mm lateral to the alar facial groove, 2 mm lateral to the first injection point in the same horizontal plane, and 2 mm inferior and between the first two sites.[19]
Orthognathic Surgery
Dentoalveolar or orthognathic surgery becomes the only alternative in some severe cases of vertical maxillary excess: LeFort osteotomy, or maxillo-mandibular reposition, combining LeFort and Obwegeser mandibular osteotomy and surgical orthodontic treatment.[4]
Differential Diagnosis
The excessive gingival display does not have a differential diagnosis; however, it is essential to differentiate between the conditions that cause the gingival overexposure.
Prognosis
Most cases of gummy smiles can significantly improve with the available treatment alternatives, but the amount of reduction of the gingival excess will depend on its cause. Some cases will easily resolve with less invasive procedures – botulin toxin, hyaluronic acid – but with results only last for some months. Others will require surgery, achieving permanent results.
Complications
An excessive gingival display is an aesthetic concern that interferes with patients’ self-esteem and psychological status.[17] Gummy smiles can be a cause of embarrassment, leading to patients hiding or controlling their smiles.[17]
Deterrence and Patient Education
- Excessive gingival display is considered an aesthetic problem.
- The treatment is determined by the cause of the excessive display.
- It is important to manage patients' expectations regarding treatment results.
- Patients must be aware of possible complications of treatment and consent to it.
Enhancing Healthcare Team Outcomes
An attractive smile results from a harmonious relationship between the teeth, the extent of the gingival display, and the lip framing while smiling.[20] Dental professionals must not underestimate the crucial role related to the amount of gingival display in configuring an appealing smile. While the general dentist is almost always involved in the care of patients with excessive gingival display, it is essential to consult with an interprofessional team of specialists, including periodontists, oral surgeons, orthodontists, and oral and maxillofacial surgeons for the most challenging cases. The treatment outcomes of a gummy smile depend on the cause. However, to improve results, prompt consultation with an interprofessional group of specialists is recommended.