Introduction
The most anterior region of the head is the face. The human face is a unique aspect of each individual. The face contains many structures that contribute to the display of emotions, feeding, seeing, smelling, and communicating. One of the most distinguishing qualities of the face is that it is used for personal identity from person to person. Identity is essential since the face is usually the first aspect of a human that is noticeable during encounters with other individuals.
Structure and Function
The anatomy of the face can divide into three main regions: upper face, middle face, and lower face. The entire face is covered by skin superficially, while the deep anatomy contains muscles, fat pads, nerves, vessels, and bones.
Upper Face
The region that is considered the upper face starts from the hairline superiorly and ends just under the lower eyelid. The lateral borders of the upper face terminate around the temporal region. The upper face region contains the forehead, eyes, and temporal region.
Forehead
The forehead is the superior region of the upper face region. The superficial layer of the forehead is made up of skin. Deeper to the skin layer of the forehead is the fat pads. The central forehead fat pad is in the center of the forehead. Laterally to the central forehead pad is the middle forehead fat pad. The middle forehead fat pad is superior to the orbits. The fat pad that makes up the most lateral region of the upper face is the lateral temporal fat pad. The lateral temporal fat pad overlies the temporal regions and spans inferiorly to the angle of the mandible.
The muscular layer of the upper face is underneath the fat pads. The procerus muscle occipitofrontalis muscle, depressor supercilii muscle, and corrugator supercilii muscle form the majority of the forehead, while the temporal part contains the temporalis muscle. The procerus muscle is shaped like a pyramid and spans from the inferior part of the nasal bone to the middle part of the forehead. The procerus muscle is situated between the eyebrows and attaches to the frontalis muscle. The contraction of the procerus muscle allows for the elevation of the eyebrows. The occipitofrontalis muscle spans the majority of the forehead. The occipitofrontalis muscle originated from the galea aponeurosis superiorly and inserts and blends into the orbicularis oculi muscle. When the occipitofrontalis muscle contracts, it elevates the eyebrows and wrinkles the forehead. The depressor supercilii muscle originates from the medial orbital rim and inserts at the medial part of the bony orbit. The action of the depressor supercilii muscle is to depress the eyebrows. The corrugator supercilii muscle is a small muscle that originated from the supraorbital ridge and inserts on the skin of the forehead close to the eyebrows. The contraction of the corrugator supercilii muscle results in the wrinkling of the forehead. The temporalis muscle originates from the parietal and sphenoidal bone. The temporalis muscle inserts on the coronoid process and the retromolar fossa. The contraction of the temporalis muscle results in the elevation and retraction of the mandible.
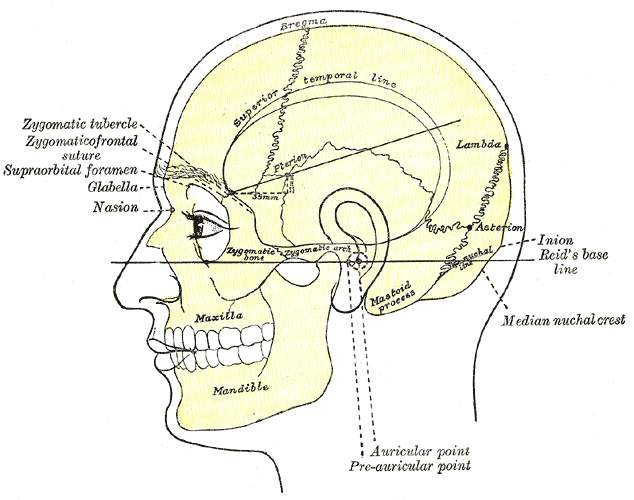
The bony structure of the forehead is made up of the frontal bone predominantly, while the lateral region of the upper face that corresponds to the temporal part forms from the temporal and sphenoid bone.
Eyes
The eyes situate in the orbital sockets in the upper face region. The skin that is directly superior to the orbits is also the region where the eyebrows are found. Surrounding and covering the eyes are the eyelids. The eyelids divide into the upper and lower eyelids. At the edges of the eyelids are the eyelashes. The eyelids cover and provide eyes with protection. Deep to the skin over the eye region are the fat pads. The superior fat pad is superior to the orbit, but inferior to the eyebrows, while the inferior orbital fat pad is inferior to the orbit and it contributes to the fullness in the superior cheek region. Laterally to each orbit is a lateral orbital fat pad.
There is one muscle that encircles the orbit. The muscle that encircles the orbit is the orbicularis oculi muscle. The orbicularis oculi muscle originated from the frontal bone, lacrimal bone, and medial palpebral ligament. The orbicularis oculi muscle inserts into the lateral palpebral raphe. The function of the orbicularis oculi muscle is to close the eyelids. In contrast, the muscle that opens the eyelids is the levator palpebrae superioris muscle. The levator palpebrae superioris muscle is not on the face but rather is in the orbital socket. Eye movement is under the control of six muscles. The six muscles that control the eyes are the superior rectus muscle, inferior rectus muscle, medial rectus muscle, lateral rectus muscle, superior oblique muscle, and the inferior oblique muscle.
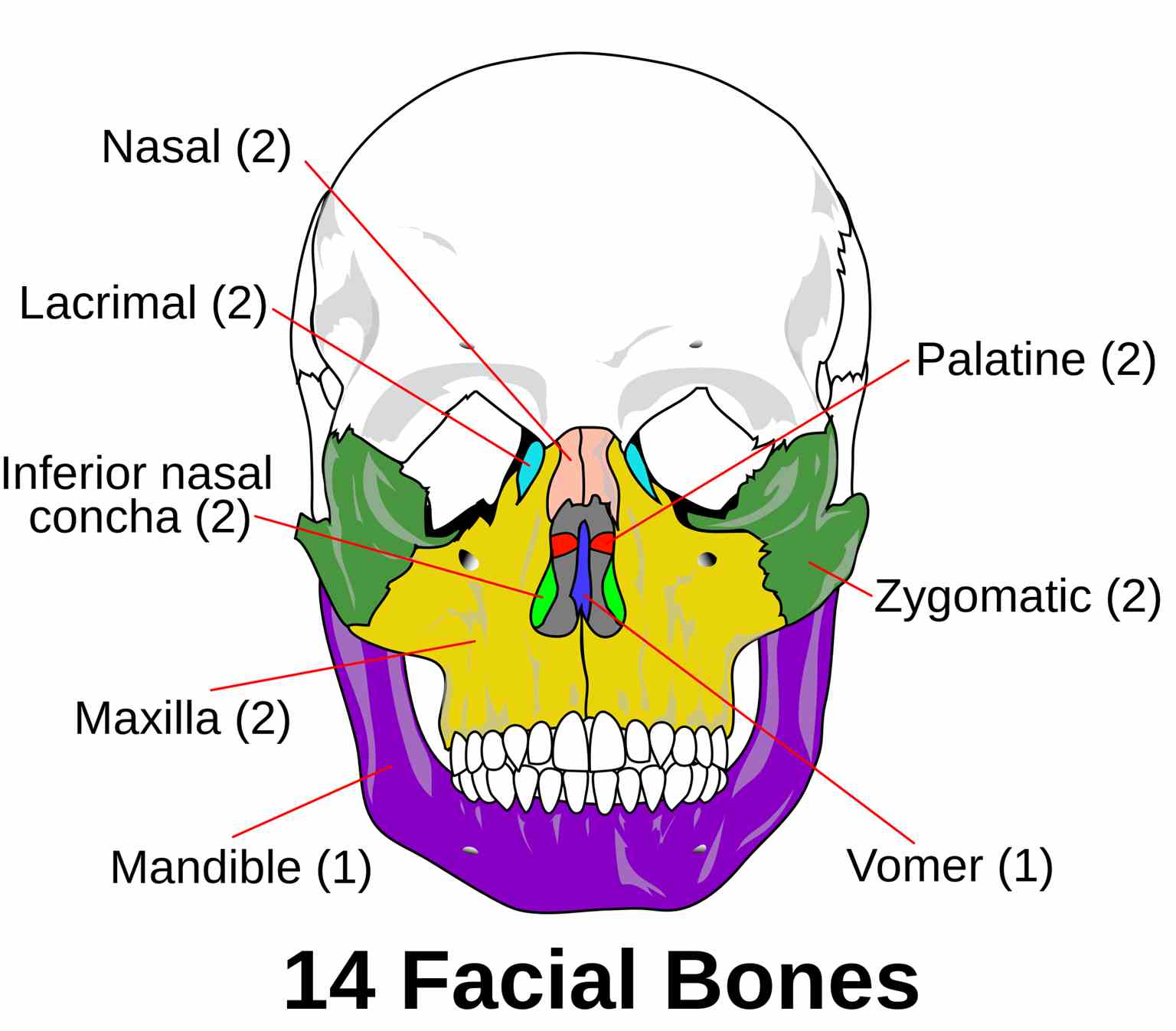
The bony structures that make the eye region are the frontal bone superiorly, nasal bone medially, maxilla inferomedially and the zygoma makes the inferior and the lateral part of the orbit.
Middle Face
The middle face region starts superior at the lower eyelid and spans inferior terminating just above the upper lip. The ears enclose the lateral borders of the central face. The central face region contains the nose, cheeks, and ears.
Nose
The nose is a midline structure that protrudes from the face. This protuberance is made from cartilage predominantly. But the base of the nose is made from the nasal bones. The nose is covered with skin superficially and has no underlying fat pads. The bony part of the nose has the nasalis muscle on top of it. The action of the nasalis muscle is to depress the tip of the nose, compression of the nasal bridge, and elevation of the nostrils. At the nasal septum, there is a muscle called the depressor alae nasi muscle. The depressor alae nasi muscle originates from the incisive fossa of the maxilla and inserts into the nasal septum. The action of the depressor alae nasi muscle is to depress the nasal septum and constriction of the nostrils.
Cheeks
The cheeks are lateral to the nose. The cheeks are covered with skin superficially, but deep to the skin, the cheeks contain a lot of fat pads. The most medial fat pad in the cheek region that demarcates the nose from the cheek is the nasolabial cheek fat pad. Just lateral to the middle cheek fat is the superficial medial cheek fat. The superficial medial cheek fat is directly inferior to the inferior orbital fat pad. More laterally, the middle cheek fat pad is lateral to the superficial cheek fat pad. The superficial cheek fat pad meets the inferior extension of the lateral temporal fat pad. The cheek region also contains a buccal fat pad that overlies the buccal muscle.
The muscular layer of the cheek contains many muscles. The cheek contains a muscle called the levator labii superioris alaeque nasi muscle. The levator labii superioris alaeque nasi muscle demarcates the medial part of the cheek and separates it from the nose. The levator labii superioris alaeque nasi muscle starts from the medial orbital wall, runs along the nostrils, and attaches to the upper lip. The action of the levator labii superioris alaeque nasi muscle is to elevate the upper lip and flares the nostrils. Just lateral to the levator labii superioris alaeque nasi muscle is the levator labii superioris muscle. The levator labii superioris labii muscle originates from the infraorbital margin and insets at the upper lip. The levator labii superioris muscle's action is to elevate the upper lip. Slightly lateral to the levator labii superioris muscle is the zygomaticus minor and major muscles. The zygomaticus minor and major muscles originate from the zygomatic angle. The zygomaticus minor muscle inserts into the skin of the upper lip. The action of the zygomaticus minor muscle is to elevate the upper lip. As for the zygomaticus major muscle, it inserts into the modiolus of the mouth. The action of the zygomaticus major muscle is to draw the angle of the mouth superiorly and laterally. There is a small muscle lateral to the zygomaticus major muscle called the levator anguli oris muscle. The levator anguli oris muscle originates from the maxilla and inserts into the modiolus of the mouth. The action of the levator anguli oris muscle is to assist in smiling by elevation of the angle of the mouth. Underneath, the zygomaticus muscles lie the buccinator muscle. The buccinator muscle originates from the alveolar process of the maxilla and mandible, buccinator crest, and temporomandibular joint. The action of the buccinator muscle is to compress the food against the buccal mucosa during mastication. Laterally, to the buccinator and zygomaticus muscle is the masseter muscle. The masseter muscle originates from the zygomatic arch and the maxillary process on the zygomatic bone, and then it inserts at the ramus of the mandible. The action of the masseter muscle is to elevate and protrude the mandible during mastication. The masseter muscle and the region anterior the ear contains the parotid gland superficially. The parotid gland produces digestive enzymes and is the structure the facial nerve penetrates before it divides into five nerve branches.[1]
The bony structure that makes the cheek region is the maxilla bone.
Ears
The lateral structures that outline the middle face region are the ears. The ears are made from cartilage and function to funnel in sound. The ears have three muscles that act on it. The muscles that act on the ears are the auricular muscles (anterior, posterior, and superior). The auricular muscles originate from the galea aponeurosis and inserts onto the helix and pinna of the ear. The action of the auricular muscles is to wiggle the ears.
The bone structure that allows for the ears to protrude from is the temporal bone.
Lower Face
The lower face starts superiorly at the upper lip and ends inferiorly at the lower border of the chin. The lateral border of the lower face is made up of the angle of the mandible. The lower face region contains the lips, chin, and jaws.
Lips
In the lower face region, the lips are the most noticeable structures in the area. The lips divide into the upper and lower lips. The function of the lips is for the articulation of speech, eating, kissing, and sensory structures. The orbicularis oris muscle surrounds the lips. The orbicularis oris muscle is a sphincter muscle that originates from the mandible and maxilla then inserts onto the skin of the lips. The action of the orbicularis oris muscle is to alter the shapes of the lips for eating, speaking, kissing, and more. In the lower face region, the risorius muscle inserts into modiolus at the angle of the mouth but originates from the parotid fascia. The action of the risorius muscle is to pull the angles of the mouth back. Most of the muscles in the lower face region will act predominantly on the lower lip. The medial region of the lower lip has two sets of paired muscles. These muscles are the mentalis and the depressor labii inferioris muscle. The mentalis muscle originates from the anterior mandible and inserts onto the chin. The action of the mentalis muscle is to protrude the lower lip, elevate, and wrinkle the skin of the jaw, while the depressor labii inferioris muscle originates from the mandible and inserts onto the lower lip. The action of the depressor labii inferioris muscle is to depress the lips. At the angles of the mouth, the depressor anguli oris muscle lies. The depressor anguli oris muscle originates from the tubercle of the mouth and inserts into the modiolus of the mouth. The action of the depressor anguli oris muscle is to depress the angle of the mouth.
The bony structures of the lips are made from the maxilla superiorly and the mandible inferiorly.
Chin and Jaw
The chin is also called mental protuberance. This structure appears on the midline of the mandible. The chin has a pre-mental fat pad that is close to the tip of the chin, while the jaw and jawline form from the lateral portions of the mandible. The jawline has the inferior jowl fat pad just lateral to the pre-mental fat pad. There is a small fat pad superior to the inferior jowl fat pad, and its called the superior jowl fat pad. The lower border of the chin and jawline have the platysma muscle. The platysma muscle is a superficial muscle that originates from the infraclavicular and supraclavicular regions then inserts onto the mandible, cheek, and mouth. The action of the platysma muscle is to depress the corners of the mouth and pull the neck skin superiorly. The platysma muscle also acts as a protective muscular layer for the vital structures such as the trachea, esophagus, carotid arteries, jugular veins, and nerves that are beneath the platysma muscle.
Embryology
During the development of the fetus, the external human face starts to develop during the fourth through sixth weeks. The face derives from the first two pharyngeal arches, neural crest cells, frontonasal prominence, medial nasal prominence, oropharyngeal membrane, and lateral nasal prominence. During week four of development, the oropharyngeal membrane breaks down to create the oral cavity. The frontonasal prominences develop into the forehead, bridge of the nose, medial nasal prominences, and lateral nasal prominences. The medial nasal prominences will further develop into the primary palate, philtrum, upper four incisors, and parts of the jaw. The lateral nasal prominences develop into the sides of the nose. The first pharyngeal arch will form the cheeks, lateral upper lip, lateral upper jaw, and secondary palate. The second pharyngeal arch will form the lower lip and jaw. All these structures form bilaterally and migrate toward the midline before fusing.[2]
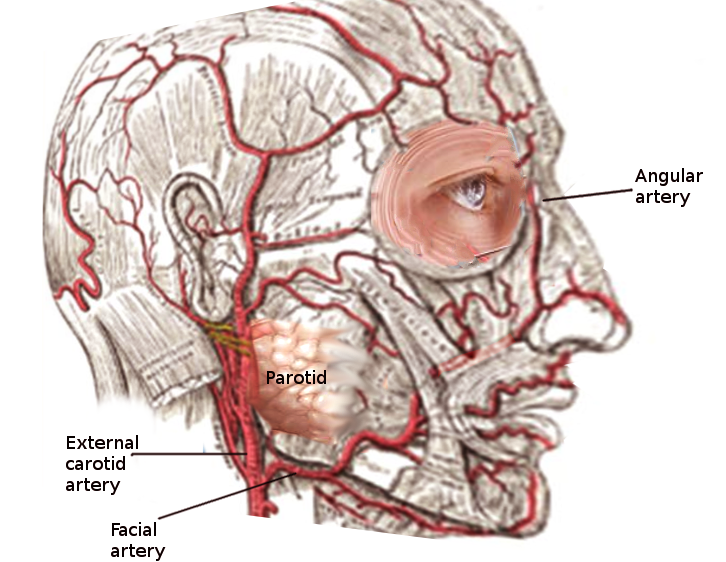
The nerve innervation of the face will also originate from the first and second pharyngeal arches. The first pharyngeal arch will form the trigeminal nerve, while the second pharyngeal arch develops the facial nerve. As for the blood supply to the face, the third aortic arch forms the common carotid artery, which divided into the internal and external carotid arteries as it elongates. As the external carotid artery elongates, it further branches into the superior thyroid, lingual, facial, ascending pharyngeal, occipital, posterior auricular, and superficial temporal arteries. Uniquely, the first aortic arch forms the maxillary artery that perfuses the deeper structures of the face. The maxillary anastomoses with the external carotid artery becoming one of the terminal arterial branches of the external carotid artery.
Blood Supply and Lymphatics
The primary blood supply to the face derives from the external carotid artery and the branches of the external carotid artery. As the common carotid artery ascends cranially, it branches into the internal and external carotid arteries. The external carotid artery further branches into superior thyroid, lingual, facial, ascending pharyngeal, occipital, posterior auricular, maxillary, and superficial temporal arteries. The facial, superficial temporal, and maxillary arteries are the main vessels that will provide perfusion to the face. The superficial temporal artery travels toward the temporal and forehead region. The superficial temporal artery perfuses the structures mainly in the temporal and forehead territories. The facial artery is responsible for perfusing the majority of the face. The facial artery travels toward the nose and lips, while the maxillary artery provides some perfusion to the cheek region. The maxillary artery travels toward the deep structures and perfusing the deeper facial structures.[3][4] As for the venous drainage, the face drains the majority of the venous blood via the facial vein. The facial vein eventually drains the blood back into the internal jugular vein.
The lymphatic drainage of the face is dependent on the location on the face. The nasal region contains facial lymph nodes, while the region closer to the ears and angle of the mandible contain preauricular lymph nodes. The lymph in the face tends to drain to submental, submandibular, and cervical lymph nodes depending on which is closer. The right side of the face will eventually drain into the right lymphatic duct while the left side will drain into the thoracic duct. The right lymphatic duct and the thoracic duct then drain back into the central circulation.
Nerves
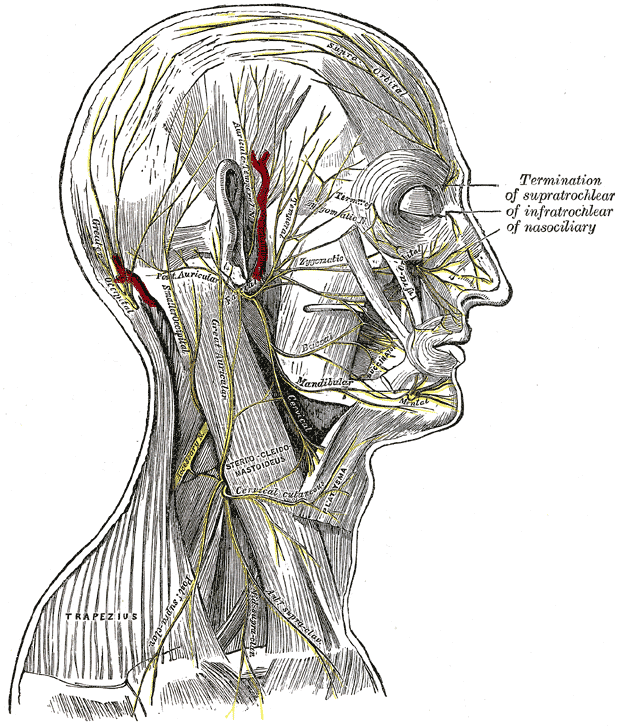
The face has two main nerve innervations. The nerves that innervate the face are cranial nerves. The facial nerve is responsible for the innervation of the muscles that participate in facial expression. The facial nerve penetrates through the parotid gland and then branches into five nerves: temporal, zygomatic, buccal, marginal mandibular, and posterior cervical nerve. The temporal branch of the facial nerve travels toward the temporal and forehead region. The zygomatic branch of the facial nerve travels along the zygoma and cheek region. The buccal branch of the facial nerve travels toward the buccal region. The marginal mandibular branch of the facial nerve travels toward the mandible. Lastly, the posterior cervical branch of the facial nerve travels toward the cervical region. These nerve branches provide motor innervation to the facial muscles that are near their corresponding paths/territories.[5]
As for the sensory innervation of the face, the trigeminal nerve proves the sensory innervation to the face. The trigeminal nerve branches into three nerve branches. These branches are the ophthalmic, maxillary, and mandibular nerves. The ophthalmic nerve travels toward the forehead and provides sensory to the forehead and eye region. The maxillary nerve travels toward the maxilla bone and provides sensory innervation to the cheek and nose. The mandibular nerve travels with the mandible and provides sensory innervation to the jaw and lips. The trigeminal nerve also innervates the masseter muscle that contributes to the fullness of the cheeks. The eyes also receive additional innervation from the optic, oculomotor, trochlear, trigeminal, abducens, and facial nerves. The nose also receives special sensory innervation from the olfactory nerve. Lastly, the ears funnel in sound and convert it into audible sound via the vestibulocochlear nerve.[6]
Muscles
These are the muscles located on the face.
- Occipitofrontalis muscle
- Temporalis muscle
- Procerus muscle
- Nasalis muscle
- Depressor septi nasi muscle
- Orbicularis oculi muscle
- Corrugator supercilii muscle
- Depressor supercilii muscle
- Auricular muscles (anterior, superior and posterior)
- Orbicularis oris muscle
- Depressor anguli oris muscle
- Risorius muscle
- Zygomaticus major muscle
- Zygomaticus minor muscle
- Levator labii superioris muscle
- Levator labii superioris alaeque nasi muscle
- Depressor labii inferioris muscle
- Levator anguli oris muscle
- Buccinator muscle
- Mentalis muscle
- Platysma muscle
- Masseter muscle
Most of these muscles receive innervation from the facial nerve and participate in facial expression except for the masseter muscle. The innervation of the masseter muscle is via the trigeminal nerve, and this muscle participates in mastication.
Physiologic Variants
The face is one of the most variable structures in humans. The face represents the identity of each person. Unfortunately, some individuals are born with congenital defects that alter the appearance of their face. And others suffer injuries or diseases that affect the way their face appears. And others alter the appearance of their faces with cosmetics products and procedures. The human face can also change over time as a person ages. The environment and lifestyle of an individual can manifest in changes in the face. For instance, a person exposed to UV light will have darkening of the skin, while an individual that consumes an excessive amount of calories may gain fat content in their face. For this reason, the human face is extremely variable, but the standard features such as the eyes, nose, and mouth are consistently present in most individuals.
Surgical Considerations
Anatomy of the face is essential when it comes to surgeries in the face. The face is highly vascularized and heavily innervated by nerves. The knowledge of the anatomy of the face can guide clinicians in the avoidance of damage to crucial structures in the face during surgeries and injections in the face.
Forehead lift, also known as a brow lift, is a surgical procedure that some individuals receive to decrease the appearance of wrinkles across the forehead, bridge of the nose, and between the eyes. A plastic surgeon usually performs this surgery. The procedure consists of removing segments of excess skin and fat to reduce the appearance of wrinkles.[7]
Cheek augmentation is a cosmetic procedure that enhances the appearance of the cheeks by adding volume, removing sagginess, or removing wrinkles. The augmentation of the cheeks can be done by implantation of cheek implants or the injection of fillers to add volume to the cheeks. The addition of implants or injected fillers will increase the volume of the cheeks, usually resulting in less sagging and wrinkling of the cheeks.
Otoplasty is a surgical procedure done to correct or alter the ear. This surgery is done to improve the proportions and position of the ear to make a face appear more desirable to the patients.[8]
Rhytidectomy is also known as a facelift. This procedure reduces the appearance of the wrinkles and sagging skin from aging. In a facelift, the surgeon may remove excess fat pad and resect excess sagging skin to create a tighter and more defined face.[9]
Lower rhytidectomy is also known as a neck lift. This procedure targets the platysma muscle. The resection and tightening of the skin on the neck make the neck appear more desirable and hides the features of aging in some individuals.[10]
Buccal fat removal is a procedure where the buccal fat pad is removed to create the illusion of dimpling and a more defined cheekbone.[11]
Mentoplasty is a procedure done to enhance the appearance of the chin by implants or resection of the chin. The decision to resect or to add chin implants is decided by the patient on what would make them appear more natural or enhanced.
Blepharoplasty is a procedure done to alter the appearance of the eyelids. This procedure can reduce the appearance of bags under the eyes, eye puffiness, wrinkles due to excess skin, or reduction of excess skin that is obstructing vision.
Facial implants are done to enhance the appearance of the cheeks, chin, or jaw by the placement of implants. Implants are done to enhance and make the various regions appear fuller with less wrinkling.
Rhinoplasty is also known as a nose job. Rhinoplasties are done to alter the appearance of the nose to make it appear more proportionate to the dimensions of the face.
All of these procedures are also useful in conjunction with facial trauma repairs. In facial traumas, the surgeons operate to repair and restore the appearance of the patient's face. Sometimes the cosmetic procedures are done as adjunctive in facial trauma repairs to optimize the surgical approach to the restoration of the face.
Clinical Significance
The face is a structure in the human that is commonly affected by dermatological disease and conditions. Many dermatological disorders appear in the face, such as acne vulgaris, neoplasms, rashes, sun damage, and more. The various skin diseases in the face are treated based on the underlying etiologies.
The appearance of the face can also be used to guide treatment in patients since the face can show clinicians the patient's mood through facial expressions. For example, pain can appear as grimace in the face, and happiness present by smiling, and anger can also be visible in the face. These distinctions in the human face can guide in tailoring the patient's care accordingly. Also, the face can appear flushed when the patient has an elevated temperature. The phenomenon of facial flushing is due to the dilation of blood vessels in the face. The reason for this noticeable flushing is due to the dense vascularity of the face. Many etiologies can result in a flush face, but this can be one sign that can further guide a clinician in narrowing his or her differential diagnoses.
Other Issues
The face is a structure that is heavily innervated by nerves. Any disturbances in the innervation of these nerves will manifest as defects in the face. One example is the middle cerebral artery (MCA) infarction. This may manifest as contralateral drooping and impaired sensation of the face sparing the forehead. These clinical features can guide clinicians in the diagnosis of an MCA stroke, while complete unilateral drooping of the face can present in Bell palsy. These differences are useful to determine the etiologies of the conditions.