Continuing Education Activity
Chest trauma poses a significant threat to patient health and survival due to potential vital organ damage in the involved area. This type of trauma is the second most common form of unintentional traumatic injury and ranks third in terms of mortality among patients with polytrauma. Studies indicate that up to 60% of chest trauma cases are fatal, emphasizing the urgency for prompt evaluation and intervention. Elucidating the injury mechanisms, whether penetrating or blunt, is crucial for effective management. Rapid recognition of life-threatening conditions such as tension pneumothorax and hemothorax is paramount, with stabilization taking precedence according to Advanced Trauma Life Support protocols. Collaborative efforts involving emergency clinicians, surgeons, anesthesiologists, and intensive care unit clinicians are vital for optimizing patient outcomes.
This activity for healthcare workers is designed to enhance learners' competence in evaluating and managing chest trauma. Participants gain deeper insights into evidence-based guidelines and best chest trauma management practices, including resuscitation algorithms, imaging protocols, and surgical interventions. Learners become equipped to collaborate effectively with an interprofessional team, improving outcomes for patients with chest trauma.
Objectives:
Identify the signs and symptoms indicating possible hemodynamic compromise in patients with chest trauma.
Create a clinically guided diagnostic plan in patients with chest trauma.
Apply evidence-based guidelines for selecting appropriate surgical interventions in patients with chest trauma.
Implement optimal interprofessional communication and coordination strategies to develop comprehensive short- and long-term management plans for patients with chest trauma.
Introduction
Chest Trauma Overview
Chest trauma represents a significant challenge in emergency medicine and trauma care, encompassing a broad spectrum of injuries ranging from minor rib fractures to life-threatening thoracic organ damage. Accidents, falls, assaults, and motor vehicle collisions (MVCs) are common chest trauma etiologies.
Chest trauma is the second most frequently occurring unintentional traumatic injury and the third most common cause of death after abdominal injury and head trauma in patients with polytrauma.[1] Chest trauma results in the highest mortality, reaching up to 60% in some studies.[2] In patients with severe trauma, 25% of deaths are due to chest trauma.[3] Thus, this condition is a leading contributor to morbidity and mortality worldwide.
Injury to any vital midthoracic organ can progress rapidly. Prompt recognition, assessment, and appropriate management of chest trauma are essential to mitigate associated complications and improve patient outcomes.
Anatomy of the Midthoracic Region
A thorough grasp of the pertinent anatomy is paramount to managing chest trauma effectively. The thoracic cage is comprised of the sternum, ribs, and thoracic vertebrae, providing crucial structural support and safeguarding vital organs within the chest cavity. The mediastinum is the thoracic cavity's central compartment, housing vital structures like the heart, great vessels, trachea, esophagus, and lymph nodes.
The lungs are the primary respiratory organs, nestled within the pleural cavities and undertaking pivotal functions such as gas exchange, blood oxygenation, and carbon dioxide elimination. The heart is positioned centrally within the mediastinum, receiving deoxygenated blood from the venous system and ensuring the circulation of oxygenated blood throughout the body.
The great vessels facilitate systemic and pulmonary circulation. These vessels include the aorta, pulmonary artery, superior and inferior vena cavae, and pulmonary veins. The trachea and bronchial tree conduct air from the larynx to the bronchi, which further branch into smaller bronchioles and alveoli within the lungs that facilitate vital air exchange. The diaphragm, a domed muscle separating the thoracic and abdominal cavities, aids respiration through its contraction and relaxation.
The esophagus lies adjacent to the trachea and conveys food and liquids from the mouth to the stomach through peristaltic contractions. The pleural space, the potential space between the visceral and parietal pleurae, normally contains a small quantity of lubricating fluid to facilitate smooth lung movement during respiration. The visceral pleura is a thin membrane covering the lungs' surface, closely adhering to their contours. The parietal pleura lines the thoracic cavity's inner surface and is attached to the chest wall, diaphragm, and mediastinum, providing structural support to the lungs and contributing to the maintenance of negative intrapleural pressure.
The intercostal nerves run along the intercostal spaces and provide sensory innervation to the thoracic wall and motor innervation to the intercostal muscles. Phrenic nerves originate from cervical spinal nerves C3 to C5, descending to innervate the diaphragm and regulate breathing. The vagus nerve supplies various thoracic structures, including the heart, lungs, esophagus, and abdominal viscera, contributing to the regulation of vital functions like cardiac contraction, respiration, and digestion.
The sympathetic chain lies alongside the vertebral column, contributing sympathetic innervation to thoracic organs, blood vessels, and muscles. Splanchnic nerves arise from the sympathetic chain and extend into the abdominal viscera, transmitting sensory and autonomic signals between the thoracic and abdominal regions. The recurrent laryngeal nerve branches from the vagus nerve and supplies sensory innervation to the laryngeal mucosa and motor innervation to the laryngeal muscles, which are crucial for airway protection and vocalization.
Etiology
Chest trauma can result from penetrating or blunt trauma. Blunt trauma is a more common cause of traumatic injuries and may be life-threatening. The injury mechanism informs both primary and secondary surveys from the care team, especially what type of imaging modalities are indicated and when to involve a surgical consult.[4][5] MVCs are the leading cause of chest trauma. Most acute traumatic aortic injury cases also result from MVCs. Crushing or deceleration is the main cardiac injury mechanism. An open pneumothorax is associated with gunshot injuries.
Epidemiology
Chest trauma is one of the most common blunt injuries affecting patients of all ages. The 2016 Pediatric Report of the National Trauma Data Bank documented that chest injuries had the highest fatality rate by body region. MVC is the most common cause of these fatal conditions. Pulmonary contusion is more common in children compared to rib fractures.[6] Pneumothorax occurs in 30% of chest trauma.
Recent data indicates that 36% of trauma deaths in the United States are potentially preventable. Among these, thoracic injuries account for 41%, with blunt trauma as the primary mechanism (80 to 92%). Delayed treatment, inadequate management, and treatment errors are the primary causes of preventable deaths.[7]
Geriatric patients have a higher mortality compared to younger patients with similar injuries. Older patients with a single rib fracture have twice the mortality as their younger counterparts with the same injury. Mortality increases by 19% and the pneumonia risk by 27% for each additional rib fractured. Children are more prone to developing hypoxia when their functional reserve is depleted.
Pathophysiology
Blunt or Penetrating Trauma
Thoracic injury is classified into blunt and penetrating. Blunt trauma imparts kinetic energy to the point of impact and causes direct damage to the chest and more distant sites. Penetrating trauma transfers kinetic energy into the tissues involved and is related to the square of the projectile velocity. Impairments at either the chest wall, musculature, or gas exchange influence breathing.
Pneumothorax
Pneumothorax is the accumulation of air in the pleural space from a breach in the visceral or parietal pleura, leading to lung collapse and symptoms such as chest pain and difficulty breathing. Tension pneumothorax occurs due to the formation of a "flutter valve," which facilitates unidirectional airflow into the pleural space and increases pleural gas volume and pressure. An open pneumothorax may occur when chest trauma creates a communication between the chest cavity and the external environment.
Pediatric Considerations
Greater kinetic energy transfer occurs in children as their chest wall is more pliant and compressible. The pediatric mediastinum's increased mobility allows it to readily shift to the contralateral side, facilitating robust compensation until tension physiology ensues and shock manifests.
Cardiac output is relatively fixed during early life. Therefore, younger patients can remain normotensive despite significant blood volume loss. Hypotension develops when all physiological compensatory mechanisms are exhausted. Children have an increased hypoxia risk due to this cohort's lower functional residual capacity and higher tissue oxygen consumption.
History and Physical
Individuals with chest trauma may present with apnea, unresponsiveness, and inaudible cardiac tone. The primary survey must be quick, assessing the airway, breathing, circulation, disability, and exposure. Resuscitation must be immediately started, simultaneously addressing significant injuries such as hemorrhage sites. A more detailed secondary survey may be completed after stabilizing the patient.
History
Conscious patients with chest trauma may complain of chest pain, dyspnea, hemoptysis, palpitations, or sensations of pressure or tightness in the chest. Associated symptoms such as dizziness, nausea, and diaphoresis may be reported if significant bleeding or cardiac injury occurs. Pain, deformity, and loss of function in other sites may be present in polytrauma cases. Flank or abdominal pain may be elicited in patients with a concomitant abdominal injury. Individuals with esophageal injuries often present with odynophagia, dysphagia, and hematemesis. Chest or back pain may also suggest esophageal injuries. Loss of consciousness may be a sign of significant blood loss, hypoxia, or concomitant brain injury.
The injury mechanism must be explored. Chest trauma most commonly arises from MVCs, falls, assaults, and penetrating injuries. The event's circumstances, including the force direction and impact, must be noted. Extensive vehicle damage, passenger space intrusion, prolonged extrication, airbag deployment, and steering wheel damage are all risk factors for significant injury in MVCs and must be assessed during history-taking.
The patient's past medical history helps guide overall management. Medical conditions that often impact trauma interventional approaches include diabetes mellitus, cardiovascular disease, coagulopathies, chronic lung disease, immunosuppression, and renal impairment. Exploring the patient's social history, including factors like tobacco use, alcohol consumption, drug use, and occupational or recreational activities, may provide additional clues relevant to injury management. A review of systems allows for the identification of any injuries that may have occurred concurrently with the chest trauma.
Physical Examination
Physical examination findings increase suspicion of chest trauma. Early recognition of life-threatening injuries is a priority. The following conditions should be quickly identified and addressed.
- Airway obstruction or rupture
- Tension pneumothorax
- Cardiac tamponade
- Massive hemothorax
- Flail chest
When the initial exam is complete and adjunct imaging is complete, a secondary survey is indicated that may reveal the following:
- Rib fractures
- Small hemothorax
- Small pneumothorax
- Pulmonary contusion
- Chest wall contusion
Potentially serious hidden injuries requiring a higher level of suspicion include the following:
- Tracheobronchial injury
- Aortic injury
- Myocardial contusion
- Pulmonary contusion
- Diaphragmatic rupture
- Esophageal rupture
Patients with significant hemorrhage, prolonged hypoxia, or severe brain injury may be unconscious. Findings suspicious for hemodynamic instability in a conscious patient include tachycardia, tachypnea, hypotension, and hypoxemia. Tachyarrhythmias may also be noted on the cardiac monitor, either from blood loss or myocardial trauma. An aortic root disruption may lead to rapid death due to blood loss, pericardial bleeding, and tamponade.
Inspection should include evaluation for bruising, abrasions (for example, the "seat belt sign"), and penetrating wounds. Agitated or uncooperative patients may have alcoholic breath.
On auscultation, diminished breath sounds may suggest hemothorax or pneumothorax. Chest wall contusions with a seatbelt pattern may produce point tenderness over the ribs. Crepitus and point tenderness on palpation signify pneumothorax or pneumomediastinum.
The diagnosis of tension pneumothorax is clinical—patients with tension pneumothorax present with respiratory distress, tachypnea, and hypoxia. Decreased or absent breath sounds occur on the affected side. The trachea is deviated away from the affected side. Neck veins may be distended. In patients with hypovolemia, the neck veins may not be distended.
Pulmonary contusion should be suspected in patients with chest wall injury, especially if presenting with hypoxia. The degree of hypoxia often correlates with contusion size.[8][9]
The physical examination must also assess for concomitant injuries. A detailed vascular examination is warranted, including bilateral pulse and upper extremity blood pressure. Patients who present unconscious but are resuscitated and stabilized require a complete neurologic examination.
Evaluation
The diagnostic process for chest trauma involves performing imaging, laboratory, and physiologic studies, aiding in timely diagnosis, risk stratification, and appropriate management to optimize patient outcomes. The choice of diagnostic tests must be clinically guided. The roles of the most important modalities are explained below.
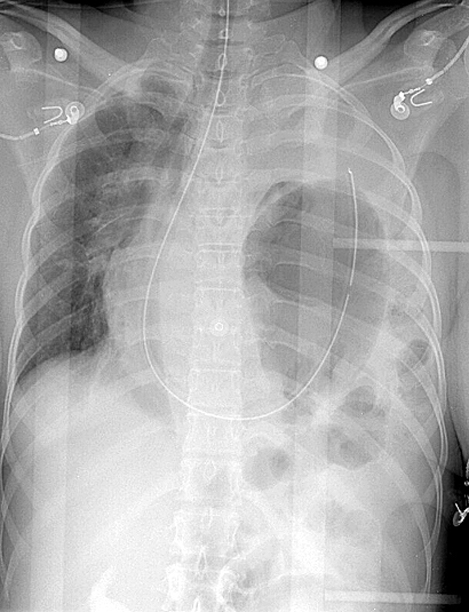
Chest Radiography
A portable chest radiograph is required in most trauma codes (see Image. X-Ray, Blunt Chest Trauma). However, the diagnosis of tension pneumothorax is clinical. If suspected, rapid decompression must be immediately performed. Radiographic confirmation is often not necessary for intervention. However, traditional physical examination indicators like tracheal deviation and distended neck veins exhibit low sensitivity when diagnosing tension pneumothorax. Point-of-care ultrasound provides accurate identification of tension pneumothorax.[10]
Small and medium-sized pneumothoraces and hemothorax may be missed in supine chest radiography. An aortic injury should be suspected in the presence of a widened mediastinum, apical capping, aortic knob loss, or left mainstem bronchus deviation. A ratio of over 25% of the chest width is useful in determining mediastinal widening. An occult pneumothorax is suspected if a deep costophrenic sulcus, hemidiaphragm hyperlucency, and an abnormally well-defined mediastinal or cardiac border are evident.[11][12][13]
Focused Assessment with Sonography in Trauma
Traditional Focused Assessment with Sonography in Trauma (FAST) has 4 views: the cardiac (subxiphoid) window, right upper quadrant (Morrison pouch), left upper quadrant (LUQ), and suprapubic (bladder) window. In contrast, the extended FAST (e-FAST) includes pulmonary views to evaluate for pneumothorax and hemothorax, besides traditional FASTS’s 4 views. This exam should be started in the area with the highest suspicion of injury. If the thorax is of concern, then eFAST should start in this area. A black collection outside an organ, viscera, or pericardia suggests the presence of free fluid in the area. Free fluid found on eFAST usually indicates the presence of blood.
The anterior chest wall areas between the ribs may be evaluated by eFAST to search for pneumothorax. Bedside eFAST is more sensitive when evaluating pneumothorax than supine chest radiography. An ultrasound probe may be placed on the chest to assess lung sliding, the absence of which suggests pneumothorax.
The spinal stripe appears as a bright line parallel to the ribs and represents a reverberation artifact produced by the interface between the ribs and the air-filled lung tissue. Finding the spinal stripe superior to the diaphragm in the right and left upper quadrant windows in an acute trauma setting helps identify hemothorax.[14][15][16][17] The eFAST should be completed during the primary survey, especially in unstable patients, to direct definitive management.
Computed Tomography
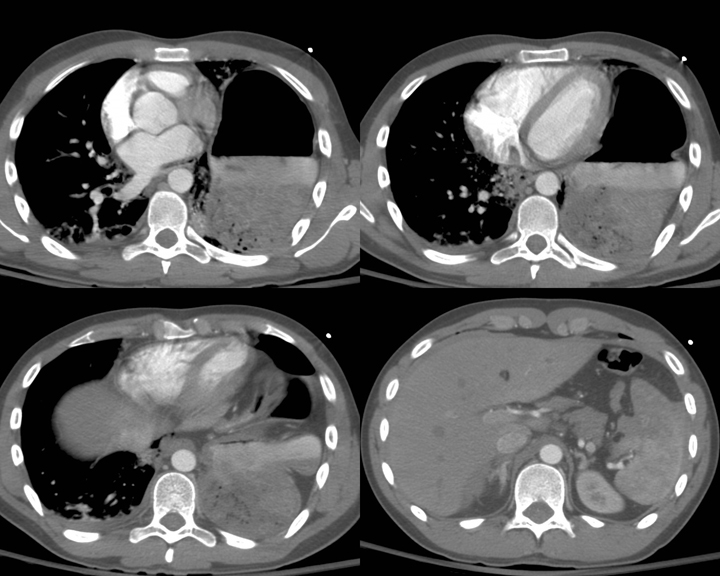
Computed tomography (CT) scan is more sensitive and specific for evaluating midthoracic structures than radiography or ultrasonography (see Image. Blunt Chest Trauma on Computed Tomography). This imaging modality is definitive in patients with chest trauma, helping to identify serious injuries more reliably. A CT scan may show pericardial effusion or hemopericardium in patients with cardiac injury. However, the patient should be hemodynamically stable throughout the test.
Spiral chest CT angiography should be obtained in patients with high-energy injury mechanisms to evaluate for aortic injury. Findings suggestive of aortic injury include intimal flaps, pseudoaneurysm formation, abnormal aortic contour, and a sudden aortic caliber change. The following classification helps assess the severity of aortic injury:
- Grade I: Intimal disruption
- Grade II: Intramural hematoma
- Grade III: Pseudoaneurysm
- Grade IV: Aortic rupture
Most aortic injuries are located at the aortic isthmus, around 2 cm distal to the left subclavian artery’s origin. An occult intimal injury should be suspected if a hematoma is immediately adjacent to the aorta without evidence of another aortic injury.
Blood Tests
Blood tests that may be crucial in evaluating patients with chest trauma include a complete blood count, coagulation studies, blood typing, arterial blood gases, cardiac enzymes, and blood glucose.
The complete blood count can help identify anemia, which may indicate acute blood loss. Leukocytosis suggests infection or inflammation. Thrombocytopenia may be observed in patients with significant bleeding or disseminated intravascular coagulation. Coagulation studies may reveal abnormalities in clotting function and guide appropriate management to minimize bleeding complications. Blood typing helps identify compatible blood products for potential transfusion in significant hemorrhage cases or if surgery is contemplated.
Arterial blood gas analysis provides valuable insights into respiratory function and acid-base balance in patients with hypoxemia or shock. Cardiac biomarkers may be indicated if a myocardial injury is suspected, ie, based on clinical presentation and electrocardiography (ECG). Glucose levels should be monitored in patients who are unconscious or with a known history of diabetes mellitus.[18]
Electrocardiography
ECG assesses for potential cardiac involvement in acute trauma settings. This modality can help identify conduction abnormalities, myocardial ischemia, and signs of cardiac contusion. Specifically, findings such as ST-segment elevation or depression, T-wave abnormalities, new-onset bundle branch blocks, or dysrhythmias may indicate cardiac injury. However, a normal ECG does not rule out cardiac injury. Additional imaging studies and clinical evaluation are often necessary to assess patients with chest trauma comprehensively.
Imaging Adjuncts
Imaging adjuncts include endoscopy and bronchoscopy to assess for esophageal and pulmonary injuries, respectively.[19][20] A CT scan followed by an esophagogram should be obtained to determine esophageal injury if a chest wound is near the esophagus.
Major thoracic trauma rarely occurs in isolation. Associated injuries are often present. Some injuries are challenging to diagnose and require increased suspicion, such as traumatic aortic injury, tracheobronchial disruption, and traumatic diaphragmatic tear.
Treatment / Management
Injury-specific interventions are required following the primary survey, prioritizing airway, breathing, and circulation stabilization. Prompt interventions, such as emergent chest tube thoracostomy (CTT), are necessary for managing immediate life-threatening injuries, including large pneumothoraces and hemothorax. Patients with pneumothorax should receive 100% oxygen via a nonrebreather mask, with needle decompression followed by CTT if tension pneumothorax is suspected. In hemothorax cases, adequate drainage is imperative to prevent blood retention in the pleural space. Retained hemothorax can lead to empyema requiring video-assisted thoracoscopic surgery.[21]
Most thoracic trauma cases can be managed nonoperatively. However, operative management should not be delayed when warranted. Operative thoracic injury exploration should be considered if initial (CTT) drainage exceeds 1000 to 1500 mL, approximately 200 mL per hour for 2 to 4 hours is drained, or hypotension of unknown cause continues despite resuscitation by blood transfusion. Asymptomatic, stable patients with an occult pneumothorax may not require a CTT. Patients with occult pneumothoraces rarely progress to tension physiology.[22]
Admission
Patients with 3 or more rib fractures, a flail segment, and any number of rib fractures with pulmonary contusions, hemopneumothorax, hypoxia, or preexisting pulmonary disease should be hospitalized. These patients should be monitored at an advanced care level.
Pain Control
Pain management is critical in reducing respiratory complications.[23] Pain control significantly affects mortality and morbidity in patients with chest trauma.[24] Pain leads to splints—involuntary guarding due to pain—which worsen or prevent healing. In many cases, splints can lead to pneumonia. Early analgesia should be considered to decrease splinting.
Push doses of short-acting narcotics may be given in the acute setting. Other pain control options include intrapleural nerve blocks, transdermal patches, intravenous analgesia, and epidural analgesia.
Nonnarcotic transdermal patches are a safe option and should be considered when chest wall pain persists despite a lack of confirmed rib fractures, an adjunct pain control modality is required, or the patient is discharged.
Antibiotics
A study revealed that prophylactic antibiotics for CTT performed under sterile conditions in blunt thoracic trauma did not reduce the incidence of pneumonia or empyema. Such findings suggest that routine prophylactic antibiotic use may not be necessary in all chest trauma cases where CTT is performed, and their benefits must be evaluated alongside their potential risks, such as antibiotic resistance and adverse reactions.[25]
Operative Management
A careful evaluation is required to identify patients who require surgical intervention. Open reduction and internal fixation has been shown to decrease mortality in patients with flail chest, shorten the duration of mechanical ventilation, reduce hospital stay, and reduce intensive care stay.[26] Most pulmonary contusions require supportive therapy until the contusion heals. Contusions can gradually evolve over the first 24 to 48 hours after trauma. Thus, close monitoring is needed. Treatment aims to prevent respiratory insufficiency, failure, and complications.[27] Appropriate pain control helps avoid chest muscle splinting that may limit lung expansion.
Supportive care like postural drainage, suctioning, chest physiotherapy, incentive spirometry, encouraging coughing, and deep breathing are attempted to prevent atelectasis. Bilevel or continuous positive airway pressure may be used for positive pressure ventilation.[28] Minimum positive end-expiratory pressure is necessary to keep the lungs open, recruit maximum alveoli, and prevent barotrauma.[29] Prone positioning of the patient with contusion reduces stress on the diaphragm, and positioning the contused lung in a nondependent position helps recruit alveoli.
Noninvasive ventilation can cause significant gastric distention and aspiration if consciousness is impaired. Invasive ventilation is required if positive pressure ventilation fails. Low tidal volumes are suggested, as large tidal volumes can have adverse effects. Patients with severe hypoxia and poor response to other therapies can benefit from nitric oxide. Diuretics reduce pulmonary venous resistance and capillary hydrostatic pressure, thus improving contusions. Measuring pulmonary artery pressure is recommended to maintain euvolemia while avoiding pulmonary edema when administering fluid therapy.
Surgical stabilization of multiple rib fractures or flail chest corrects pulmonary mechanics. Extracorporeal gas exchange has been successfully used for pulmonary contusions refractory to all conventional therapies.[30] Surgical repair is required for aortic injuries with pseudoaneurysm formation.
Aortic Injuries
Aortic injuries are managed based on severity. Conservative management is usually attempted for Grade I injuries. Grade II injuries are monitored closely for a few days using appropriate imaging modalities, such as CT aortography, magnetic resonance orthography, or transoesophageal ultrasound. Surgery is performed if the condition progresses. Grade III to IV injuries require emergent intervention, although most patients with Grade IV aortic injury do not survive before hospital arrival.[31]
Esophageal Injuries
Esophageal injuries should be managed early and aggressively. Gastrointestinal contents may contaminate the mediastinum through a torn esophagus and lead to complications such as mediastinal abscess and sepsis.[32] Additionally, delayed management of esophageal injuries can lead to difficulties with swallowing and oral intake.
Differential Diagnosis
The following differential diagnosis should be considered in patients presenting with chest trauma:
- Acute coronary syndrome: Chest pain or pressure often radiates to the left arm or jaw and is associated with dyspnea, diaphoresis, and nausea. Susceptible patients may develop this condition in acute traumatic settings, as it may be precipitated by significant bleeding or emotional stress.[33]
- Pneumonia: Chest pain is exacerbated by coughing or deep breathing and is associated with fever, productive cough, and signs of respiratory distress.
- Pulmonary embolism: This condition presents with sudden-onset pleuritic chest pain worsened by deep breathing and accompanied by dyspnea, tachypnea, and signs of hemodynamic instability. Risk factors include prolonged immobility and coagulopathies.
- Aortic dissection: This condition presents with severe, sudden-onset chest pain radiating to the back. Dyspnea, hypotension, and signs of aortic regurgitation or peripheral ischemia may be present.
- Tension gastrothorax: Chest pain and difficulty breathing arise due to the presence of a gastric herniation into the thoracic cavity, leading to lung tissue compression and mediastinal shift.
- Pericarditis: Chest pain is exacerbated by deep breathing or lying flat and is associated with dyspnea, fever, and a pericardial friction rub.
- Anxiety or panic attack: Chest pain, palpitations, and hyperventilation may develop after chest trauma.
- Musculoskeletal pain: Chest pain is exacerbated by movement or palpation and is not associated with dyspnea or other respiratory symptoms.
A thorough clinical assessment and diagnostic testing can help distinguish chest trauma from these conditions.
Prognosis
The outcomes of chest trauma vary depending on the extent of injury. The prognosis for isolated rib fractures is good. However, lung or cardiac injury often leads to prolonged recovery. Thoracic aortic injuries are life-threatening and generally associated with poor outcomes. These injuries are independent predictors of mortality. Most patients may die before reaching an emergency department, and many patients who reach the hospital die within 24 hours.
The highest morbidity following chest trauma is seen in younger and older patients.[34] Chest trauma is one of the leading causes of pediatric mortality.
Complications
Complications of chest trauma include pneumonia, acute respiratory distress syndrome, acute lung injury, mediastinitis, arteriovenous fistula, and bronchopleural fistula. These conditions may be due to direct damage or secondary to critical injuries.
Consultations
Consider a lower threshold for trauma activation, especially in cases of penetrating chest injuries. Stable patients with chest trauma should be examined by the surgeon on duty.
Thoracic surgeons should be involved early to consider surgical management of specific injuries. Immediate thoracic surgical intervention is required in the following situations:
- Initial blood loss of at least 1,500 mL or greater than 200 mL/hour over 2 to 4 hours
- Massive contusion with significant ventilatory impairment
- Tracheobronchial tree injury
- Vascular injury, including the heart or large vessels
The collaborative involvement of the interprofessional team, comprising healthcare professionals such as surgeons, emergency physicians, and critical care specialists, facilitates comprehensive evaluation and timely intervention. This approach ensures effective care coordination and optimized treatment strategies for patients with chest trauma.
Deterrence and Patient Education
Chest trauma prevention involves a multifaceted approach addressing primary and secondary prevention strategies. Primary prevention focuses on mitigating risk factors and promoting safety measures to prevent traumatic events, such as implementing strict seatbelt and helmet use laws, promoting safe driving practices, enforcing speed limits, and reducing exposure to violence and physical altercations. Additionally, workplace safety protocols, including proper personal protective equipment use in high-risk occupations, can help prevent occupation-related chest trauma.
Secondary prevention strategies aim to minimize the severity of injuries when traumatic events occur. Preventive measures include prompt access to emergency medical services, effective prehospital care, and public education on first aid techniques. Chest trauma severity and incidence can be significantly reduced by prioritizing injury prevention measures at individual, community, and societal levels.
Pearls and Other Issues
The key points when evaluating and managing chest trauma are as follows:
- Patients should be stabilized first before performing definitive surgical intervention. Airway, breathing, and circulation must be examined and addressed according to Advanced Trauma Life Support guidelines.
- Injuries likely to arise from a chest trauma mechanism must be identified or anticipated. Blunt and penetrating chest injuries present with different symptom patterns.
- Thoracic trauma rarely occurs in isolation. Other body areas must be investigated for associated injuries. Life-threatening injuries must be rapidly recognized and addressed.
- The presence of a flail chest signifies severe thoracic injury. Significant chest trauma can occur without rib fractures.
- High-velocity chest injuries are associated with lung contusion, pneumothorax, hemothorax, and intrathoracic blood vessel damage.
- The presence of rib fractures may suggest that significant force has been applied. The underlying structures must be evaluated. Lower rib fractures may be associated with intraabdominal injuries.
- Pneumothorax can occur in both blunt and penetrating thoracic trauma. A simple pneumothorax can progress to a tension pneumothorax.
- Pulmonary contusion often occurs in patients with chest wall injury. The contusion may be silent during the initial evaluation. Hypoxia is the most important clinical sign of pulmonary contusion.
- Plain chest radiography may reveal vascular injury, including hemothorax, wide mediastinum, and loss of aortic knob contour.
- The trauma team must be activated promptly in the presence of hemodynamic instability. Stable patients with thoracic injuries warrant a surgical consultation.
- Aortic injuries are managed based on severity.
- Esophageal and cardiac injuries must be treated promptly and aggressively.
Improving safety on the road, at work, and at home prevents traumatic injuries. However, trauma prevention efforts must come from different sectors of society to be truly effective.
Enhancing Healthcare Team Outcomes
Chest trauma is best managed by an interprofessional team comprising emergency physicians, trauma surgeons, anesthesiologists, thoracic surgeons, intensive care clinicians, cardiac surgeons, nurses, respiratory therapists, and pharmacists. The emergency physician initially assesses and stabilizes patients with chest trauma and coordinates the subsequent care pathway. Trauma surgeons offer their expertise in surgical interventions for severe thoracic injuries and oversee the overall management of trauma patients. Anesthesiologists ensure optimal pain management and airway control, particularly during surgical procedures or in critically ill patients requiring mechanical ventilation.
Thoracic surgeons bring specialized skills in the surgical management of complex chest injuries, including chest wall reconstruction, lung resection, and repair of thoracic vascular injuries. Intensive care clinicians provide comprehensive critical care management for severely injured patients, including hemodynamic stabilization, ventilatory support, and monitoring for potential complications. Cardiac surgeons may be involved in cases of cardiac trauma, providing surgical management of cardiac injuries or complications arising from thoracic trauma.
Nurses are essential in chest trauma management, providing initial assessments, interventions, and ongoing monitoring to stabilize patients. Respiratory therapists provide respiratory support interventions such as oxygen therapy, airway management, and mechanical ventilation to ensure adequate oxygenation and ventilation in patients with chest injuries. Pharmacists collaborate with healthcare teams to optimize medication regimens and provide valuable patient education on medication use and potential side effects.[35] Through coordinated efforts and expertise from each team member, the interprofessional team ensures comprehensive and effective management of chest trauma, leading to improved patient outcomes.